How much testosterone should I take to feel normal again without wrecking my health?
Too little and you feel nothing.
Too much and you risk side effects, mood swings, and long-term issues.
Finding the right TRT dosage isn’t about chasing high numbers. It’s about steady levels, symptom relief, and lab results that make sense.
There’s no single “perfect” number that works for everyone.
Age, body fat, metabolism, and delivery method all change your ideal TRT dosage.
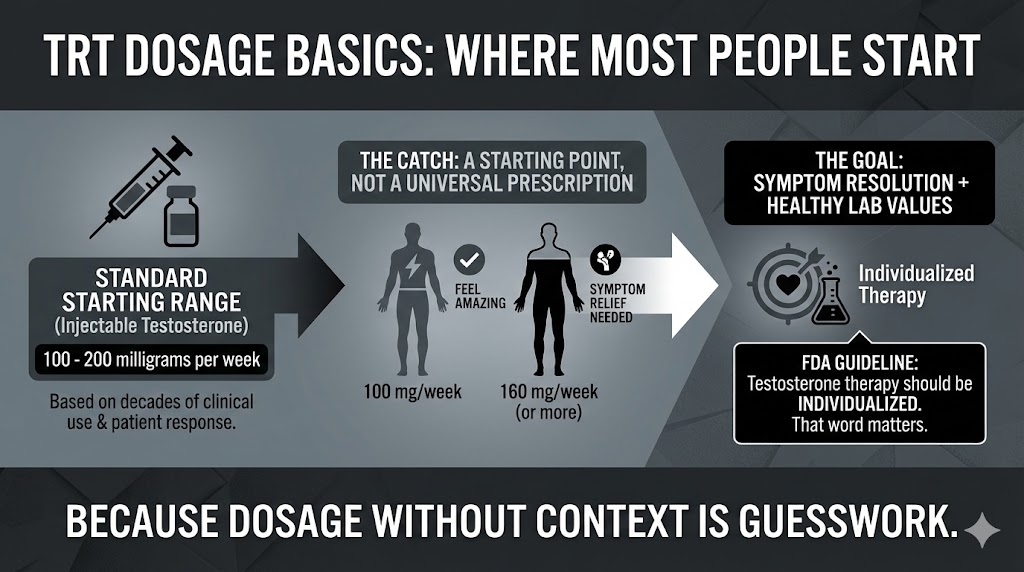
TRT Dosage Basics: Where Most People Start
If you’re brand new to therapy, you’ll notice that most providers begin with a standard TRT dosage range. For injectable testosterone, that often means 100 to 200 milligrams per week. That’s not random. It’s based on decades of clinical use and patient response.
But here’s the catch. That range isn’t a prescription for everyone. It’s a starting point. Some men feel amazing at 100 mg per week. Others need closer to 160 mg to see symptom relief. The goal isn’t the dose itself. The goal is symptom resolution with healthy lab values.
Not all testosterone delivery systems behave the same. Your TRT dosage depends heavily on how you administer it.
With injections, weekly dosing is common. Many patients split their weekly TRT dosage into two smaller injections to keep levels steady. For example, instead of 160 mg once per week, they inject 80 mg twice weekly. That often reduces mood swings and energy crashes.
Topical gels are different. A typical gel TRT dosage might range from 50 to 100 mg applied daily. Absorption varies by person, so bloodwork becomes even more important.
Pellets work on longer cycles. Providers calculate pellet insertion amounts based on body weight and baseline testosterone levels. Adjustments only happen every few months.
TRT Dosage and Bloodwork: The Numbers That Actually Matter
Here’s where people mess up.
They chase a high number on their lab sheet instead of dialing in the right TRT dosage for their body. Total testosterone matters, yes. But so do free testosterone, estradiol, hematocrit, and SHBG.
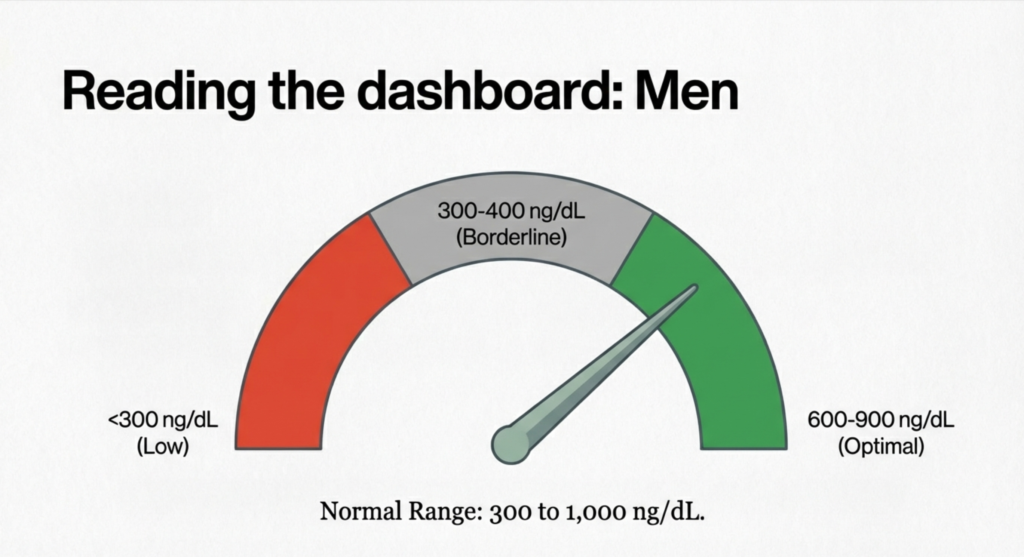
Most providers aim for total testosterone levels between 600 and 900 ng/dL. That’s a common target zone. But some men feel their best at 550. Others don’t feel relief until 850. That’s why adjusting TRT dosage based on symptoms plus labs makes more sense than labs alone.
Because guessing your TRT dosage without labs is like driving blindfolded. It might work for a mile. Then it won’t.
Adjusting TRT Dosage: When and Why Changes Happen
Most people don’t nail their ideal TRT dosage on day one. And that’s normal.
Adjustments happen for three main reasons. First, symptoms persist. Maybe energy improved but libido didn’t. Second, labs drift out of range. Hematocrit might climb. Estradiol might spike. Third, side effects appear.
When that happens, providers don’t usually double your dose. They tweak it. A small 10 to 20 mg shift in weekly TRT dosage can make a big difference. Patience matters here. Hormone levels stabilize over weeks, not days.
That transition period is where most confusion happens.
And here’s my hot take. If a clinic never checks your labs or never adjusts your TRT dosage, that’s a red flag. Therapy should evolve with you.
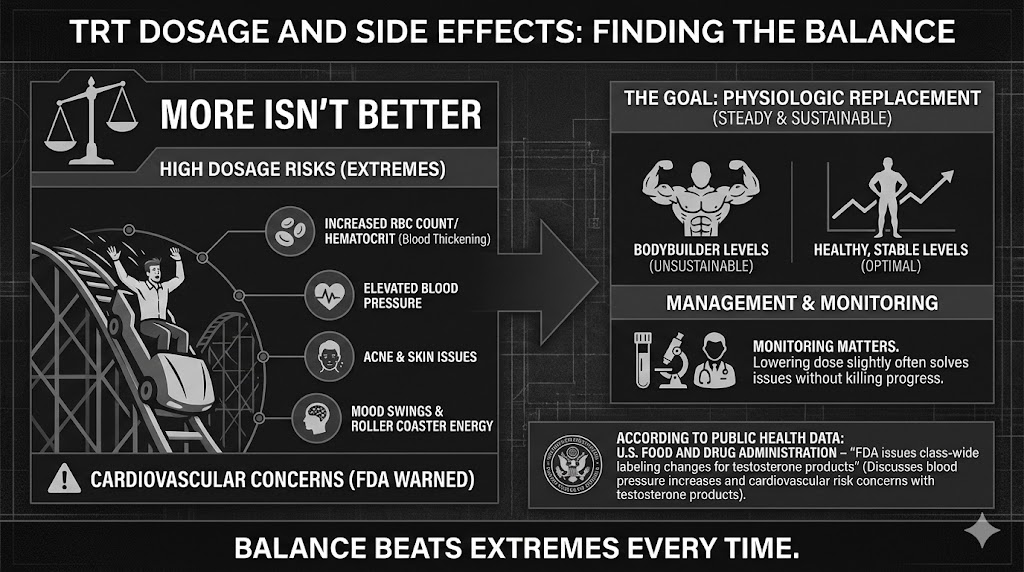
TRT Dosage and Side Effects: Finding the Balance
More isn’t better. I’ll say it again. More isn’t better.
High TRT dosage levels can increase red blood cell count, blood pressure, acne, and mood swings. You might feel strong for a while. Then you feel irritable. Or tired again. That roller coaster usually points to dosing issues.
Elevated hematocrit is common with aggressive TRT dosage plans. That’s why monitoring matters. Sometimes lowering the dose slightly solves the problem without killing your progress.
According to public health data: U.S. Food and Drug Administration – “FDA issues class-wide labeling changes for testosterone products” (discusses blood pressure increases and cardiovascular risk concerns with testosterone products)
Extremely high testosterone levels carry cardiovascular concerns.
Your goal isn’t bodybuilder levels. It’s physiologic replacement. Steady. Sustainable.
Balance beats extremes every time.
TRT Dosage for Different Age Groups
Age plays a role in how your body responds to TRT dosage, but not in the way most people assume.
Younger men with clinically low testosterone may respond quickly to moderate dosing. Older men often metabolize hormones differently and may require smaller adjustments to maintain stable levels.
That doesn’t mean older patients automatically need less TRT dosage. It means monitoring becomes even more important. Liver function, cardiovascular risk, and overall health shape dosing decisions.
Some providers use weight-based formulas when calculating initial TRT dosage, especially for pellets. Others prefer symptom-driven titration.
TRT Dosage Myths
Myth one: Higher TRT dosage equals faster muscle gain. Not true. Gains depend on training, diet, sleep, and genetics. Testosterone helps, but it’s not magic.
Myth two: Everyone should aim for 1,000 ng/dL. Why? That number looks impressive. But it’s not required for symptom relief in most men.
Myth three: You should feel amazing in one week. Hormones take time. Your body needs weeks to adapt to a new TRT dosage.
Here’s the truth. Smart therapy is boring. Consistent labs. Small adjustments. Gradual improvement.
Because guessing leads to frustration. Strategy leads to results.
Conclusion: TRT Dosage Is Personal, Not One-Size-Fits-All
If you take one thing from this guide, let it be this: TRT dosage is not a fixed number. It’s a process.
Your ideal TRT dosage depends on symptoms, labs, delivery method, and how your body responds over time. Most men start between 100 and 200 mg per week with injections, or equivalent dosing in gels or pellets. From there, small adjustments shape the outcome.
Don’t chase extreme numbers. Don’t compare your dose to someone on a forum. Focus on steady energy, improved mood, healthy labs, and long-term safety.
Work with a provider who monitors you. Test regularly. Adjust patiently.
Because the right TRT dosage isn’t about being high. It’s about feeling like yourself again — consistently, safely, and for the long run.
BMI & GLP-1 Eligibility Checker | Do You Qualify for Weight Loss Medication?
Free Assessment Tool
BMI & GLP-1 Eligibility Checker
So you’ve been hearing about these GLP-1 medications. Ozempic, Wegovy, Mounjaro. Maybe from your doctor, maybe from that one coworker who won’t stop talking about it. Fair enough. Put in your numbers below and we’ll tell you, in about thirty seconds, whether you might be a candidate. We won’t ask for your email. We’re not those people.
1 Your Measurements
lbs
cm
kg
Please fill in all measurement fields.
2 Health Conditions
Select any conditions that currently apply to you:
Medical Disclaimer: This is a screening tool. It is not your doctor. It does not know you personally. It runs on math and general guidelines. Only a licensed healthcare provider can actually tell you whether GLP-1 medication is right for you, after looking at your whole health picture. Please talk to a real human doctor before starting anything new.
What Are GLP-1 Medications?
Let’s start with what’s already happening inside you. After you eat a meal, your gut releases a hormone called glucagon-like peptide-1. GLP-1, for short. This hormone does a few useful things: it tells your brain, “Hey, we’re good, we’ve eaten,” it keeps your blood sugar in check, and it slows down how fast food leaves your stomach. A pretty good system, actually. Your body came up with it on its own.
Now. GLP-1 medications take that same idea and turn it way up. They were originally made for people with type 2 diabetes, which makes sense, since the hormone helps regulate blood sugar. But then something interesting happened. Patients started losing weight. Not a little weight. A lot of weight. Enough weight that researchers said, “Huh. We should probably study that.” And they did.
What these drugs do, basically, is flood your system with a synthetic version of that hormone at levels your body would never produce on its own. The result: your appetite drops, your cravings quiet down, you feel full for longer after meals, and your blood sugar behaves itself. For a lot of people, this combination adds up to the kind of weight loss they’d been trying to get for years through willpower alone. Which, as many of us know, has its limits.
The names you’ve probably seen are semaglutide (that’s Ozempic and Wegovy, same drug, different labels) and tirzepatide (Mounjaro and Zepbound). Tirzepatide is a bit of an overachiever. It targets two hormones instead of one, GIP and GLP-1, which might explain why it tends to produce slightly better numbers in clinical trials. But both are real, and both work.
Who Qualifies for GLP-1 Weight Loss Treatment?
Here’s where it gets practical. The rules for who can get these medications are, thankfully, not that complicated. There are basically two doors in:
Pathway 1
BMI of 30 or Higher
If your BMI is 30 or above, that’s the obese category, and you generally qualify. No extra conditions needed. Just you and your number.
Pathway 2
BMI of 27+ With a Health Condition
BMI between 27 and 29.9? You can still get in, but you need a plus-one: a weight-related condition like type 2 diabetes, high blood pressure, high cholesterol, or sleep apnea.
Now, these are the general guidelines. Your doctor, being your doctor, will also want to look at the bigger picture. What have you tried before? What runs in your family? What meds are you already on? What do you actually want out of this? All fair questions. And worth mentioning: insurance companies sometimes have their own ideas about who qualifies, which may or may not line up with what the clinical guidelines say. Such is the world we live in.
How Is BMI Calculated?
BMI. Body Mass Index. It’s a number. It takes two things you know about yourself, your height and your weight, and squishes them together into a single figure that doctors then use to make decisions about you. Is it a perfect system? No. It can’t tell the difference between a person who deadlifts four hundred pounds and a person who has never seen the inside of a gym. But it’s the system we’ve got, and it’s the one your doctor will use when deciding whether to write you a prescription.
BMI = weight (lbs) ÷ height (in)² × 703
Imperial formula | Metric: weight (kg) ÷ height (m)²
Let’s say you’re 5’8″ and 200 pounds. That gives you a BMI of about 30.4, which places you, just barely, into the obese category. A word that carries a lot of weight (no pun intended, or maybe a little intended). Here are the categories:
BMI Range
Category
Below 18.5
Underweight
18.5 to 24.9
Normal weight
25.0 to 29.9
Overweight
30.0 to 34.9
Obese (Class I)
35.0 to 39.9
Obese (Class II)
40.0 and above
Obese (Class III)
The thing to remember is that this number is a starting point, not the whole story. A bodybuilder might register as obese. A thin person might be carrying dangerous amounts of fat around their organs and come back “normal.” Bodies are weird and complicated and don’t always cooperate with formulas. Your doctor knows this. That’s why they’ll look at BMI alongside everything else they know about you before making any calls.
How Much Weight Can You Lose on GLP-1 Medications?
Okay, so, the numbers. People always want the numbers. And honestly? The numbers are worth wanting.
In the STEP trials, people taking semaglutide 2.4 mg (Wegovy) lost, on average, 15 to 17% of their body weight over about sixteen months. If you weigh 250 pounds, that’s roughly 37 to 42 pounds. Not nothing. Not nothing at all.
Tirzepatide (Zepbound) went further. In the SURMOUNT-1 trial, people on the highest dose lost an average of 22.5% of their body weight over 72 weeks. More than a third of them lost over 25%. To put that in perspective: those are numbers that, until recently, you only saw after someone had surgery. And these people were getting a weekly injection.
Now, before you start planning your new wardrobe. Everyone is different. Your results will depend on your dose, what you eat, how much you move, how consistent you are, and about a thousand other things your body decides on its own. These medications are a tool. A very good tool. But they work best when you also do the other stuff: eat better, move more, check in with your doctor regularly. They’re not a magic wand. (Though, if we’re being honest, they’re closer to a magic wand than most things that have come before them.)
Frequently Asked Questions
The short version: BMI of 30 or higher, you’re in. BMI of 27 to 29.9, you can still get in, but you need a weight-related health condition riding along with you. Think type 2 diabetes, high blood pressure, high cholesterol, sleep apnea. Your doctor makes the final call.
Ozempic and Wegovy are the same drug, semaglutide, wearing different name tags. Ozempic is approved for type 2 diabetes. Wegovy is approved for weight loss. Same with tirzepatide: Mounjaro is the diabetes version, Zepbound is the weight loss version. Tirzepatide targets two hormones instead of one, which may be why it tends to show slightly better weight loss numbers. But both drugs are real, and both work.
If your BMI is between 27 and 29.9, having one of these conditions can get you through the door: type 2 diabetes, high blood pressure, high cholesterol, sleep apnea, heart disease. Some providers also count PCOS. Your doctor will look at your specific situation and decide what applies.
It is not. This is a calculator on the internet. A useful one, we think, but still: a calculator on the internet. Only a real, licensed healthcare provider can look at your full medical history, your current medications, your goals, your life, and tell you whether GLP-1 medication is right for you. Think of this as the first question in a longer conversation.
In clinical trials, people on Wegovy lost 15 to 17% of their body weight over about sixteen months. Zepbound at the highest dose showed averages up to 22.5% over 72 weeks. Those are averages, though. Some people lose more. Some less. It depends on your dose, your habits, your body, and how consistent you are with the whole program. The medication helps a lot. It’s not the only variable.
Stomach stuff, mostly. Nausea, vomiting, diarrhea, constipation, stomach pain. These tend to show up in the first few weeks as your body figures out what’s going on, then they usually ease up. More serious but rare side effects include pancreatitis, gallbladder problems, and kidney issues. Your doctor will monitor things and adjust your dose if you’re having a rough time.
The honest answer is: maybe. A lot of plans cover them for type 2 diabetes without much fuss. Coverage for weight loss alone is more of a mixed bag. Some insurers want prior authorization. Some want proof you’ve tried other things first. Some just don’t cover it. Your provider’s office can usually help you figure out where your plan stands and whether there are manufacturer discount programs that can help with the cost.
So. What Now?
If you got this far, you’re probably at least a little serious. Good. Our medical team can sit down with you, go over your numbers, and figure out a plan that makes sense for your body and your life. No pressure. Just a conversation.
Most younger men don’t wake up one morning with ED. Causes of ED under 40 often show up before a man is ready to name them. A lot of guys still assume erection problems belong to older men, not someone in their twenties or thirties. Yet in everyday life, plenty of younger men struggle quietly and put on a brave face.
You hear this in clinics. You hear it after a few beers. And sometimes at 2 a.m., when someone finally talks. Most men aren’t angry then. They’re uneasy. Embarrassed. Sometimes shaken after one bad night.
Here’s the part most people miss. Erectile dysfunction before forty usually isn’t about being “less of a man.” In real life, it’s messier than that. Stress, habits, hormones, and mental overload pile up little by little. Alcohol, sleep, screens, relationships, health issues — all of it stacks quietly before anyone takes it seriously.
Sometimes your body sends an early warning. Not to punish you. Just to get your attention. It can feel brutal when it lands. It can also be the jolt you actually needed.
What follows isn’t neat or glossy. It’s closer to a real conversation with someone who sees this play out in real lives, not just journal articles.
Causes of ED Under 40 and What Your Body is Saying
When you’re under forty, erections depend on a lot of things working at once. Blood flow, nerves, hormones, and your brain all have to line up in the same moment. If one piece slips, the whole thing wobbles.
In practice, stress does more damage than most men realize. High stress tightens blood vessels before you even notice. Your body flips into alert mode, which is terrible for sex. Poor sleep does something similar overnight, quietly dulling your response.
Add energy drinks, junk food, and hours of sitting, and you’ve got problems brewing long before you feel sick. Most men don’t notice until one rough night in bed makes it impossible to ignore. Then it feels sudden. Even though it wasn’t.
Your body isn’t betraying you. It’s sending a signal. A loud one.
Now, about porn. This tends to surprise patients. Heavy use doesn’t physically damage your penis, but it can retrain how your brain expects arousal to work. Screens deliver instant novelty in a way real partners never can. Real bodies move more slowly than videos. Your nervous system gets impatient.
Masturbation itself isn’t the issue. The pattern and intensity usually are. If you need extreme visuals just to stay hard, your brain might need a reset more than your body does. Guys, panic here. Still, small changes can make a difference within weeks. Cutting back feels awkward. Then things often get clearer.
Hidden health problems show up earlier than people think. High blood pressure, prediabetes, and insulin resistance appear in men who still feel “young.” Even mild blood sugar swings can blunt the nerve signals that trigger erections. Cholesterol can restrict blood flow long before you feel unwell.
Some men only learn this after struggling in bed. That moment hurts. It also pushes them to finally get checked, which can protect their heart as much as their sex life.
Psychological Pressure That Sabotages Performance
Performance anxiety rarely arrives dramatically. It usually starts after one awkward moment. Then your mind keeps replaying it like a broken loop.
Your heart races. Your muscles tense. And the erection disappears right on cue. That loop makes anxiety the real problem.
Most men try to muscle through it with willpower. That almost never works. Slowing down, breathing, and lowering expectations usually helps more. You don’t have to prove anything in your own bedroom.
That’s where relationships get tricky. If you’ve been arguing, distant, or holding resentment, your body registers that before your mind catches up. Desire doesn’t reboot like a phone after a fight.
Still, many men expect perfect performance even when emotional trust is shaky. That expectation often backfires. Reconnecting emotionally, even in small ways, often fixes things sexually without a big talk.
Cultural ideas about masculinity make this worse. A lot of men are taught they should always be ready, hard, and dominant. That’s a story, not biology. Real bodies fluctuate with stress, mood, and sleep.
Treating every soft moment as a personal failure traps you in a nasty loop. Letting that belief go feels uncomfortable at first. Then, strangely freeing.
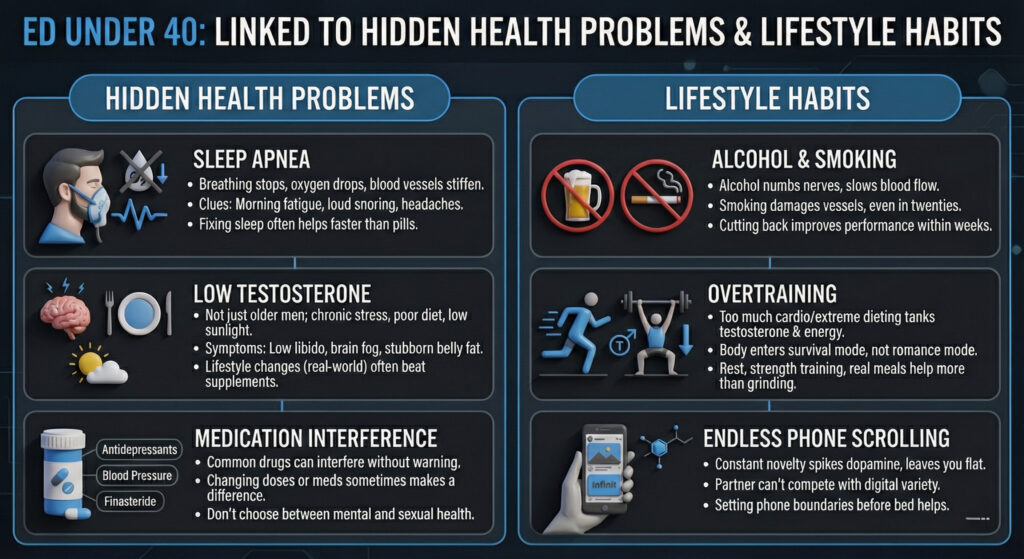
Causes of ED Under 40 Linked to Hidden Health Problems
Sleep apnea is a classic hidden culprit. Even very fit men can have it. When breathing stops at night, oxygen drops, and blood vessels stiffen. Over time, that wears down the same systems on which erections depend.
Morning fatigue, loud snoring, and headaches are common clues, but plenty of men shrug them off. Fixing sleep can help erections faster than most pills.
Low testosterone isn’t just an older man’s problem. Chronic stress, poor diet, and too little sunlight can drag levels down in younger men. Low libido, brain fog, and stubborn belly fat often show up together.
In real-world settings, lifestyle changes usually move the needle more than supplements alone. Still, some men need medical support. There’s nothing weak about that. Testing replaces guessing, which most guys quietly appreciate.
Medications can also interfere with erections without warning. Antidepressants, blood pressure drugs, and finasteride are common examples. Many doctors rush through side effects. Changing doses or medications sometimes makes a real difference. You shouldn’t have to choose between mental health and sexual health.
Lifestyle Habits That Quietly Wreck Erections
Alcohol hits harder than men like to admit. In the moment, it numbs nerves and slows blood flow. Over time, smoking damages vessels even in your twenties. A lot of guys assume they’re immune because they’re young. They’re not. Cutting back often improves performance within weeks.
Overtraining is another trap. Too much cardio or extreme dieting can tank testosterone and energy. Your body reads that as survival mode, not romance mode.
Rest days, steady strength training, and real meals usually help more than grinding harder. Bigger muscles don’t guarantee stronger erections. Not even close.
Endless phone scrolling also matters more than men think. Constant novelty spikes dopamine, then leaves you flat when real intimacy shows up. A partner can’t compete with infinite digital variety. Setting phone boundaries before bed helps, even if it feels irritating at first.
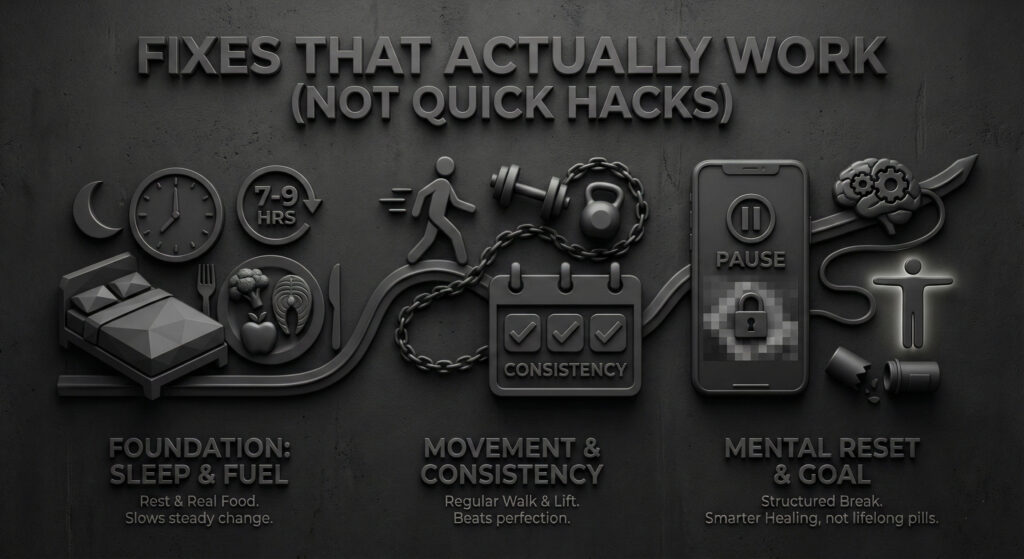
Fixes That Actually Work
Start simple before reaching for pills. Seven to nine hours of sleep most nights changes more than people expect. Real food, regular walking, and lifting a few times a week move things slowly but steadily.
It sounds boring. It still works.
Consistency beats perfection.
Taking a structured break from porn can reset how your brain responds to arousal.
The goal isn’t lifelong pills. It’s smarter healing.
Start with your partner, not just Google. Pick a calm moment, not right after sex. Say what you’re feeling without blame. Most partners respond with empathy once they understand you’re trying.
With a doctor, be specific. Explain when it started, what helps, and what makes it worse. Be honest about stress, sleep, porn, and alcohol. Doctors can’t help what they don’t know. Clear details get clearer answers.
Remember, millions of men deal with this at some point. You’re not broken or weird. You’re human. Opening up feels risky. It’s often the first real step toward change.
To Conclude!
Causes of ED under 40 almost never come from one single thing. It’s usually a slow build — stress piling on habits, habits nudging health, health shaping mindset, all of it drifting together without much warning. That can feel heavy when you finally see it. But there’s a quiet upside most men don’t clock at first: nothing here is written in stone.
Small shifts matter more than people assume. Better sleep. Real food. Moving your body in ways that don’t feel like punishment. A hard, honest talk with your partner that you’ve been avoiding for weeks. Sometimes that alone changes more than any prescription.
Here’s the part I keep coming back to. Most younger men dealing with erection problems don’t need panic, bravado, or another Google spiral at 2 a.m. They need patience, a bit of humility, and someone who tells them straight. You’re not behind. You’re not broken. Your body is talking early enough for you to do something about it.
If you listen, adjust, and keep showing up for yourself, things can shift. Slowly at first. Then more clearly. Your confidence — and your sex life — can come back stronger than you expect.
Take Control of Your Sexual Health Now
Close the tabs. Put the phone down. Especially at 2 a.m.
If any of this hits close to home, don’t sit alone with it. Explore our guides, tools, and real-world resources made for men who actually live busy, messy, imperfect lives. No hype. No quick fixes. Just practical help you can use.
Start today. One small step is enough to begin.
If something feels off, it probably is. Low T doesn’t fix itself – but we can. Contact Us Today and know for certain.
TRT stands for testosterone replacement therapy. It’s a medical treatment that restores your testosterone levels when your body stops making enough on its own. About 4 to 5 million men in the United States have clinically low testosterone, but only about 5% are getting treated for it. That’s a lot of guys running on fumes, thinking this is just what getting older feels like.
This guide is going to walk you through the whole thing—what TRT is, how it works, signs of low testosterone, what it costs, and how to get started.
What Is Testosterone Replacement Therapy?
Three words, each doing exactly what it says. Testosterone: the hormone. Replacement: putting it back. Therapy: doing so in a controlled, medical, someone-with-a-degree-is-watching kind of way.
Your body is supposed to produce testosterone on its own. The testes handle manufacturing. The brain handles management, sending signals from the hypothalamus and pituitary gland that say, essentially, “Make more” or “That’s enough.” It’s a tidy little operation. It runs in the background like a thermostat. You never think about your thermostat until the house gets cold.
But sometimes the operation slows down. The factory produces less. The management office sends weaker signals. The supply drops below what your body needs, and you feel it in your energy, your mood, your muscles, your sex drive, your ability to think clearly, and your motivation to do literally anything after 3 PM.
TRT is the medical solution. A doctor confirms your testosterone is genuinely low through blood work, prescribes a specific dose, and monitors you with regular labs to make sure levels come back to where they belong. It’s not steroids. And it’s not some masculinity supplement. It’s a correction—your body needs a certain amount of a certain thing, stopped making enough, and now a doctor is helping you get back to baseline.
This is one of the most common questions beginners have, and it’s a fair one, because from the outside the two things look similar. Both involve testosterone. Both involve needles, sometimes. But the resemblance ends there.
TRT uses small, medically supervised doses to bring your testosterone back to a normal, healthy range—typically 500 to 900 ng/dL. Anabolic steroid abuse uses doses that are 10 to 100 times higher than that to push testosterone far beyond normal levels. TRT is prescribed by a doctor, monitored with blood work, and adjusted based on how your body responds. Steroid abuse is self-administered, often stacked with other drugs, and monitored by nobody.
Think of it this way: TRT is putting the right amount of oil back in your engine. Steroids are flooding the engine and hoping the extra pressure makes you go faster. One is maintenance. The other is a gamble.
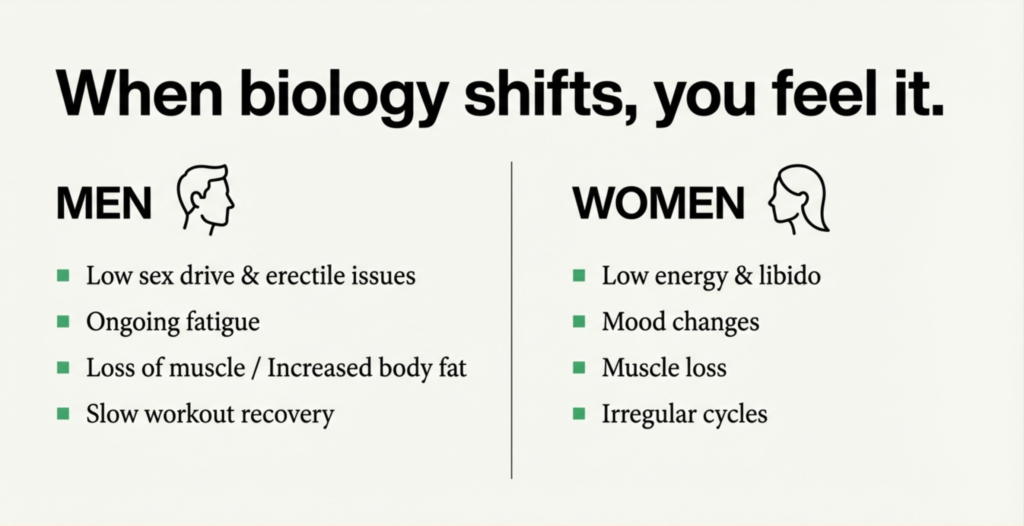
Signs and Symptoms of Low Testosterone
Here’s the tricky part. Low testosterone doesn’t show up wearing a name tag. It doesn’t tap you on the shoulder and introduce itself. What it does is much sneakier: it disguises itself as a dozen other things you already have a ready explanation for.
You’re tired all the time? Must be work. Your sex drive disappeared? Must be stress. You can’t focus? Must be your phone. You’re gaining weight around your middle? Must be age. You feel vaguely sad and you don’t know why? Must be… the news. The economy. The general condition of being a person in the 2020s.
And maybe it is those things. But low testosterone is also an explanation, and it’s one that a lot of men never consider because nobody told them to.
The most common symptoms of low testosterone include persistent fatigue that doesn’t improve with sleep, reduced or absent sex drive, difficulty getting or maintaining erections, loss of muscle mass despite consistent exercise, stubborn weight gain around the midsection, irritability or low-grade depression without an obvious cause, brain fog and poor concentration, and disrupted sleep.
If you’re reading that list and checking off three or four items and feeling a small, uncomfortable ping of recognition—that’s worth paying attention to. Not panicking about. Just paying attention to.
Normal Testosterone Levels by Age
Testosterone is measured via blood test, and the result comes back as a number in nanograms per deciliter (ng/dL). You do not need to know what a nanogram is. You just need to know where your number falls.
According to the American Urological Association, low testosterone is defined as a total testosterone level below 300 ng/dL. Your testosterone peaks in your late teens to early twenties—that period of your life when you had inexplicable confidence and terrible judgment—and then declines about 1% per year after age 30.
Here’s what the typical range looks like:
Age
Typical Total Testosterone (ng/dL)
18–25
400–700
26–35
350–650
36–45
300–600
46–55
250–550
55+
200–500
A critical nuance: the number is not the diagnosis. The number plus the symptoms is the diagnosis. A man at 310 ng/dL who feels fantastic is not a candidate for TRT. A man at 310 who hasn’t slept well in eight months and forgot what motivation feels like probably is. Context is everything.
This is the part of the guide that separates the people who are going to do something from the people who are going to bookmark this page and never look at it again. No judgment—we’ve all got a folder full of those bookmarks. A graveyard of good intentions.
But if you’re going to do something, here’s what it looks like: you ask your doctor, or a men’s health clinic, to order a testosterone blood panel. That’s the whole action item. Make a call. Schedule a lab visit.
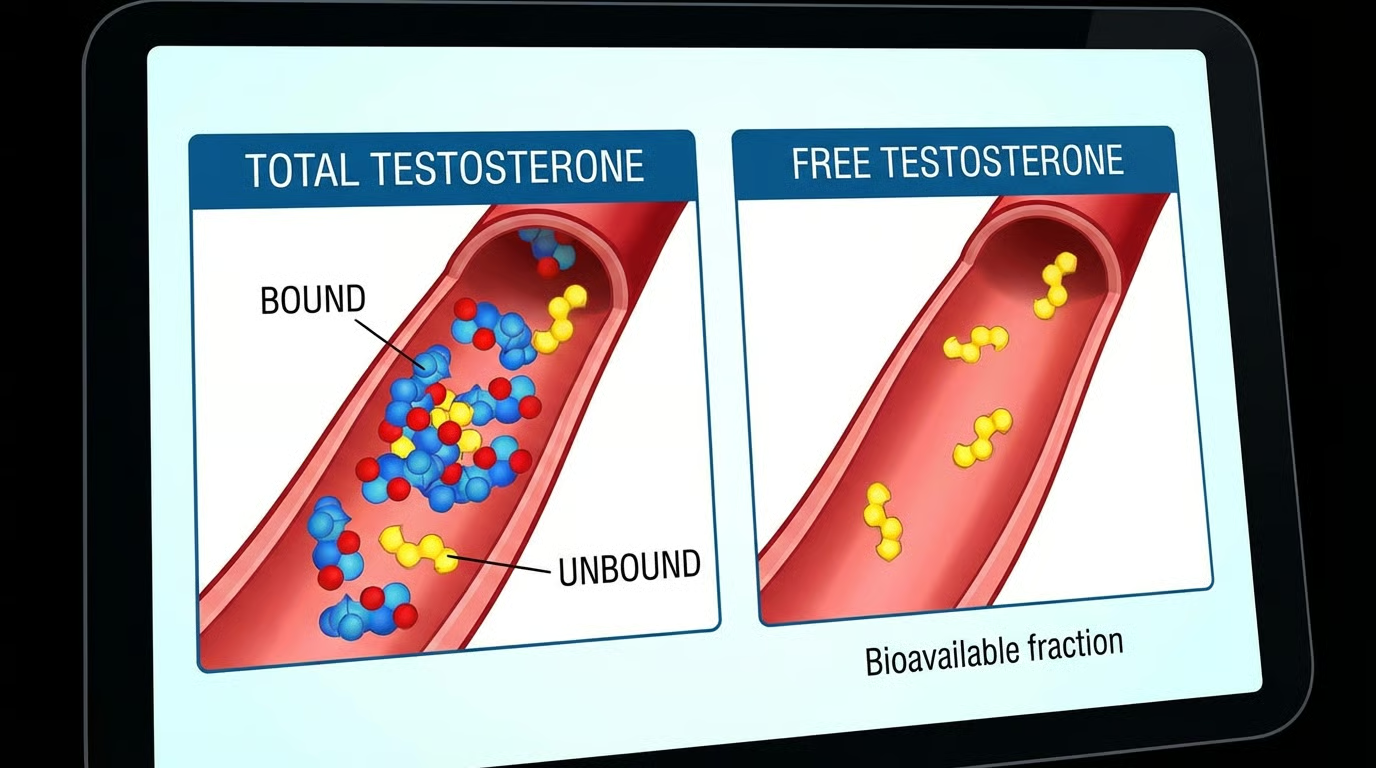
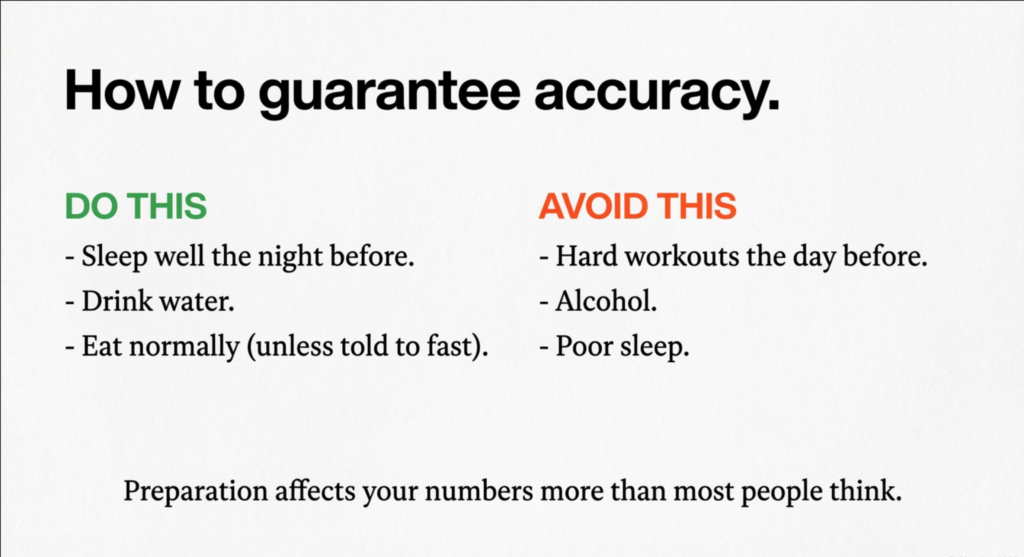
The blood draw happens in the morning—between 7 and 10 AM—because that’s when your testosterone is at its daily peak. You fast beforehand (no food, just water). The test measures your total testosterone, free testosterone (the portion your body can actually use, as opposed to the portion bound up to proteins and just riding around in your bloodstream like a passenger on a bus who fell asleep and missed their stop), and usually a handful of other markers: LH, FSH, estradiol, and a complete blood count.
One rule that matters: the American Urological Association requires two separate blood draws, on two separate mornings, both showing low testosterone, before confirming a diagnosis. One bad morning could be a fluke—stress, poor sleep, the universe messing with your lab results on that particular Tuesday. Two bad mornings means something is actually going on.
How Does TRT Work?
You’ve been diagnosed. Two blood draws. Both low. Symptoms match. Your doctor says the words “testosterone replacement therapy.” Now what?
The mechanics are simple. Your doctor prescribes a specific amount of testosterone. You take it on a regular schedule. Your levels come back up to a healthy range—the Endocrine Society’s clinical practice guidelines target 500 to 900 ng/dL. Your body starts running on the correct amount of the thing it’s supposed to be running on, and over the following weeks and months, things shift.
TRT Treatment Options
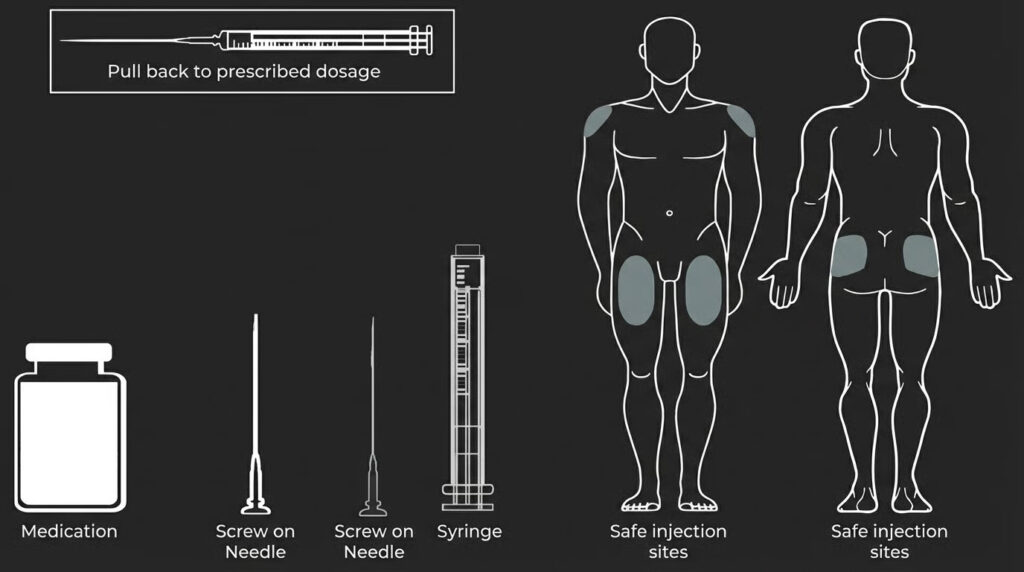
The part people really want to know is how the testosterone gets into your body. There are several options:
Method
How It Works
How Often
Intramuscular Injections (Cypionate/Enanthate)
Testosterone injected into the muscle or under the skin with a small needle. Cheapest and most common method.
1–3 times per week
Topical Gels or Creams (AndroGel, Testim)
Applied to the skin and absorbed into the bloodstream. No needles. Risk of transfer to partners/kids via skin contact.
Every day
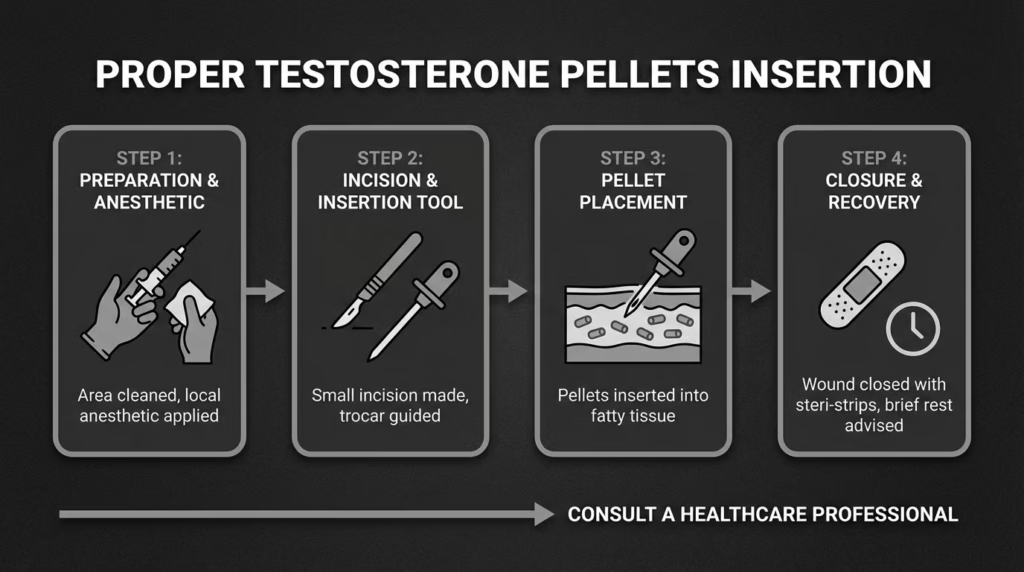
Testosterone Pellets (Testopel)
Rice-grain-sized pellets inserted under the skin in a quick office procedure. Dissolve slowly over months.
Every 3–6 months
Testosterone Patches
Medicated patch delivers testosterone through the skin. Some guys find them irritating—literally, the skin gets itchy.
Every day
Most people start with injections of testosterone cypionate. It’s the most common TRT delivery method, and it just works. It’s also the cheapest option by a wide margin and backed by more clinical data than any alternative.
TRT Results: What to Expect and When
TRT does not work like flipping a light switch. It works like a sunrise. Slowly, and then all at once, and then you look around and realize the whole room is brighter and you can’t pinpoint the exact moment it happened.
Based on clinical research, including the landmark Testosterone Trials published in theNew England Journal of Medicine, here’s what the typical timeline looks like: energy and mood improvements within 3 to 4 weeks (you don’t feel like a superhero—you feel like the version of you that doesn’t need a third coffee), improved sex drive and erectile function within 3 to 6 weeks, body composition changes (more muscle, less belly) within 3 to 6 months, and full bone density benefits within 12 to 24 months.
Your doctor will check your blood work at about 6 weeks to see how you’re responding, again at 3 months to fine-tune the dose, and then every 6 to 12 months for as long as you’re on therapy. This ongoing monitoring is not optional. It’s the thing that makes TRT safe instead of reckless.
Benefits of TRT
When testosterone replacement therapy works—and for most men with genuinely low testosterone, it does—the benefits are the kind of thing that make you wonder why you waited so long.
More energy. Not jittery, supplement-fueled energy. Just… enough. Enough to get through the day without feeling like you’re dragging a weighted sled. Your sex drive comes back from wherever it went. Your mood levels out—the unexplained irritability fades, the low-grade depression lifts. You build muscle again when you work out, instead of just getting sore. The stubborn midsection fat starts responding to things you’re already doing. Your thinking gets clearer. You sleep better.
Research supported by the Endocrine Society confirms these outcomes when TRT is administered properly and monitored with regular blood work. Not everyone experiences every benefit. But for a man who’s been operating at 60% for months or years, the collective effect can feel like getting your life handed back to you.
TRT Side Effects and Risks
Every medical treatment has potential side effects. TRT is no exception. The good news is that most are mild, predictable, and fixable by adjusting the dose. The key word is “mostly,” which is why you need a doctor watching the numbers—not a guy in a forum.
The most common TRT side effects include elevated red blood cell count (your blood gets thicker, which is why your doctor monitors something called hematocrit), acne and oily skin (usually temporary, settles within the first few months), mild water retention or bloating, breast tissue tenderness or slight swelling (happens when some testosterone converts to estrogen, which your body naturally does), and reduced sperm production.
That last one is important. If you’re planning to have kids, tell your doctor before you start. Exogenous testosterone suppresses sperm production, sometimes significantly. There are workarounds—your provider can prescribe hCG alongside TRT to maintain fertility—but only if they know about it up front.
Is TRT Safe? The Cardiovascular Question
If you’ve spent any time researching TRT online, you’ve encountered alarming headlines about testosterone and heart risk. Here’s what the science actually says.
The TRAVERSE trial, published in the New England Journal of Medicine in 2023, was one of the largest randomized controlled studies ever conducted on TRT. The finding: testosterone replacement therapy did not increase the risk of major cardiovascular events like heart attacks or strokes in men with low testosterone. In February 2025, the FDA removed its black box cardiovascular warning from prescription testosterone products based on these results. This was a landmark shift that has meaningfully reshaped how doctors evaluate TRT safety.
Who Should Not Take TRT
Testosterone replacement therapy is not appropriate for everyone. Your doctor will advise against it if you have a history of prostate or breast cancer, untreated severe sleep apnea, uncontrolled heart failure, a hematocrit above 54%, or if you’re actively trying to conceive without adjunct therapy. These aren’t necessarily permanent disqualifiers—your doctor may address the underlying issue and revisit TRT later—but they’re essential to discuss before starting.
I’m putting this section here because almost every other guide buries it or skips it, as if discussing money somehow cheapens the medical conversation. It doesn’t. You’re a grown person. You want to know what things cost. Here’s what things cost:
Treatment Type
Estimated Monthly Cost (Without Insurance)
Testosterone Cypionate (generic injectable)
$30–$80
Compounding Pharmacy Cream
$50–$120
Telehealth TRT Clinic (all-inclusive)
$150–$350
Brand-Name Gel (AndroGel, Testim)
$200–$500
Testosterone Pellets (Testopel)
$125–$335/month (inserted every 3–6 months)
The most affordable route—by a lot—is generic testosterone cypionate from a regular pharmacy. With a GoodRx coupon, you’re looking at under $30 for a vial that lasts about two months. That’s less than your streaming subscriptions.
Does Insurance Cover TRT?
Many insurance plans cover testosterone replacement therapy when you have a documented diagnosis of hypogonadism—meaning two blood tests confirming low testosterone plus clinical symptoms. Coverage varies by plan, so call your insurer and ask about formulary status, prior authorization requirements, and whether they cover monitoring labs. Even without insurance, the injectable route is genuinely affordable. The expensive versions of TRT are a choice, not a requirement.
How to Get Started with TRT
If you’re still reading—and if the thing in your chest right now is a small, cautious flicker of “this might actually apply to me”—here’s what you do. Four steps. None complicated.
Step 1: Get a blood test.
Call your doctor, go to a men’s health clinic, or use a telehealth platform. Say the words “I’d like to get my testosterone levels checked.” They’ll order a blood panel. You go to a lab in the morning, fasting, between 7 and 10 AM. Five minutes. One arm. You’ll survive it.
Step 2: Get a second blood test.
If the first result comes back low, you do it again on a different morning. Two tests, two mornings. One bad result could be a fluke. Two bad results means something is going on.
Step 3: Talk to a qualified provider.
If both results confirm low testosterone, sit down with a provider who knows what they’re doing—a urologist, an endocrinologist, a sharp primary care doc, or a reputable telehealth clinic. They’ll review your numbers, explain your options, walk through the risks, and help you decide. If at any point the provider seems uninterested in your blood work or rushes through the risks, find a different provider.
Step 4: Start treatment and follow up.
Your doctor will check your blood at 6 weeks, again at 3 months, and then every 6 to 12 months. They’ll adjust your dose based on your levels and how you feel. This is an ongoing relationship between you, your provider, and your lab results. Not a prescription you fill once and forget about.
[For a deeper dive into dosing protocols, lab monitoring, insurance details, and telehealth vs. in-person options, see our complete TRT Guide.]
Frequently Asked Questions About TRT
Is TRT the same as steroids?
No. TRT uses small, doctor-prescribed doses to restore testosterone to normal levels (500–900 ng/dL). Anabolic steroid abuse uses doses 10 to 100 times higher to push levels far beyond normal. TRT is medically supervised and monitored. Steroids, when abused, are neither as it is a Schedule III controlled substance.
How long do you stay on TRT?
For most men, TRT is a long-term or lifelong treatment. Your body reduces its own testosterone production while you’re on therapy, so stopping means your levels will drop until natural production recovers—which can take months. Some men use TRT temporarily while addressing underlying causes like obesity or sleep apnea, but the majority stay on it indefinitely under medical supervision.
Can TRT affect fertility?
Yes. Exogenous testosterone suppresses sperm production, sometimes significantly. If you’re planning to have children, tell your doctor before starting. Options like hCG (human chorionic gonadotropin) can be prescribed alongside TRT to help maintain sperm production and testicular function.
What happens if you stop taking TRT?
Your testosterone levels will drop, often below where they were before you started, because your body’s natural production has been suppressed during treatment. Most men experience a return of low testosterone symptoms. Recovery of natural production can take weeks to months. Your doctor can help you taper off safely if needed.
Do you need a prescription for TRT?
Yes. Testosterone is a Schedule III controlled substance in the United States. You need a prescription from a licensed physician, which requires a documented diagnosis of low testosterone confirmed by blood work. You cannot legally obtain testosterone for TRT without one.
The Bottom Line
Here’s the simplest version of everything you just read.
Testosterone is a hormone your body needs. Sometimes your body stops making enough. When that happens, you feel worse in a bunch of ways that are easy to blame on other things. Testosterone replacement therapy is a medical treatment that puts your levels back to normal, under a doctor’s supervision, with regular blood work to keep everything on track. It’s well-studied, it’s effective, and it’s more affordable than most people think.
The hardest part is the first part. Not the needle. Not the lab visit. The hardest part is deciding that the way you’ve been feeling isn’t just “how it is now.” It’s admitting something might be off, and that the manly thing to do isn’t to push through it—it’s to find out what’s wrong.
So if any of this sounded familiar—if you’ve been running at half-speed and calling it normal—go get a blood test. It costs you one early morning and a needle prick. If your testosterone is fine, you’ve ruled something out and you can move on. But if it’s not fine, you now know exactly what the problem is, exactly what the solution looks like, and exactly where to start.
That’s the whole point of a beginner’s guide. Not to make you an expert. Just to make sure the next step—whatever it turns out to be—is one you can take with your eyes open and your feet on solid ground.
The guys who actually fix this aren’t smarter than you. They just stopped waiting.
Limitless Alternative Medicine does the labs, the diagnosis, and the treatment plan — all under one roof, with doctors who specialize in exactly this.
When people start testosterone therapy, one question comes up fast: testosterone injections vs gel vs pellets. Which one actually works best? Which one fits your life without turning it upside down?
Here’s the thing. Most clinics talk science. Few talk real life. You don’t just want numbers on a lab report. You want steady energy. Better mood. Solid workouts. A sex drive that doesn’t disappear at 3 p.m. And you don’t want a complicated routine you’ll quit in three weeks.
This guide breaks down testosterone injections vs gel vs pellets. What each method feels like day to day, what it costs, how safe it is, and who it tends to work best for. By the end, you’ll know exactly which route makes sense for you and your schedule.
Testosterone Injections vs Gel vs Pellets vs Patches: How Each Method Works
Before comparing testosterone injections vs gel vs pellets, you need a simple picture of how each delivers testosterone into your body. They all raise levels, but the delivery system changes everything.
Injections go straight into muscle or fat. You inject once or twice weekly. Testosterone enters quickly, then slowly declines until your next dose. Think of it like refilling a tank.
Gels/Creams absorb through your skin. You rub them on daily, usually shoulders or arms. Levels rise gradually and stay fairly even, assuming you apply consistently.
Pellets are tiny implants placed under the skin by a provider. They release testosterone slowly for three to six months. No daily work. No weekly shots.
Patches are worn on the skin, usually roatetd between sites. They deliver consistent 24-hour release with consistency and stability throughout the day. No weekly shots or ups and downs on how you feel.
Testosterone Injections: The Most Popular and Cost-Effective Option
When people compare testosterone injections vs gel vs pellets, injections usually win on price and control. There’s a reason clinics prescribe them first. They work. Plain and simple.
Most men inject once or twice per week using testosterone cypionate or enanthate. You control your dose, and you can adjust fast if something feels off. Energy spikes within days. Strength returns quickly. Libido often rebounds in week one or two.
But it’s not perfect.
Some people feel “peaks and valleys.” Day two feels amazing. Day six feels flat. Splitting doses helps, but you still notice fluctuations. And yes, you’ve got to be okay with needles.
The upside? Cost. Injections are often the cheapest form of TRT. They’re also widely studied. Organizations like the U.S. Food and Drug Administration approve injectable testosterone, and it’s been used for decades.
Bottom line. If you’re comfortable learning a quick weekly routine, injections are hard to beat.
Testosterone Gel: Easy, Needle-Free, and Steady
Now let’s talk about the quieter option in the testosterone injections vs gel vs pellets debate. Gel doesn’t get flashy reviews, but some people swear by it.
You apply it every morning. Takes 30 seconds. Done.
Because it absorbs slowly through skin, hormone levels stay smoother than injections. Many users report fewer mood swings and less crash. It feels… natural. Like your body just decided to cooperate again.
Sounds perfect, right?
Well, there’s a catch. You must apply daily. Miss a day and levels dip fast. Plus, there’s transfer risk. If someone touches the application site too soon, they could absorb testosterone. That’s not great for partners or kids.
Gels also cost more than injections and insurance coverage varies. That surprises people.
Still, if needles make you tense or you want steady levels with zero medical gear, gel can be a great fit.
Testosterone Pellets: Set It and Forget It
Pellets are the wildcard in testosterone injections vs gel vs pellets. Some people love them. Others try once and never go back.
Here’s how they work. Your provider inserts small pellets under the skin, usually in the hip or glute. The procedure takes about 10 minutes. After that, testosterone releases slowly for months.
No daily gel. No weekly shots. Nothing to remember.
Honestly, that freedom feels amazing.
But there’s less flexibility. If the dose is too high or too low, you can’t easily adjust. You’re stuck until the pellets dissolve. Minor soreness after insertion is common too.
Cost tends to be higher, and you need in-office visits. Still, if convenience is everything and you hate maintenance, pellets might be worth it.
Testosterone Patches: A Middle-Ground Option Worth Considering
When people debate testosterone injections vs gel vs pellets, patches rarely get mentioned. That’s a bit unfair. They sit quietly in the middle and, for some folks, they’re actually a sweet spot.
A testosterone patch sticks to your skin and releases hormone slowly over 24 hours. You apply a fresh one daily, usually on your back, thigh, or upper arm. No needles. No messy gel. Just peel, stick, and move on with your day.
Sounds simple, right? It usually is.
Because delivery is steady, patches can produce smoother testosterone levels than weekly injections. Many users say mood and energy feel more stable, with fewer ups and downs. It’s similar to gel in that way, just less hands-on once applied.
But let’s be honest. There are trade-offs.
Skin irritation is the big one. Redness, itching, or small rashes happen more often with patches than with gels. Some people rotate sites and do fine. Others get annoyed fast and quit. Adhesion can also be tricky if you sweat a lot or train hard.
Cost usually lands between injections and gels. Not dirt cheap, but not the most expensive either. Insurance coverage varies, so it’s worth checking before committing.
So where do patches fit in the testosterone injections vs gel vs pellets decision?
They’re great if you want steady levels like gel, but without worrying about transferring medication to a partner or kids. They’re also useful for people who hate needles but don’t want daily liquid application.
Patches aren’t flashy, but they’re practical. And sometimes practical is exactly what you need.
Side Effects and Safety: What Most Clinics Don’t Explain Well
When comparing testosterone injections vs gel vs pellets, safety matters more than convenience. You don’t want great energy at the expense of your health.
All methods share similar risks. Elevated red blood cell count. Acne. Possible fertility suppression. These aren’t scary if monitored, but you must test regularly.
Bloodwork every three to six months isn’t optional. It’s how you stay safe.
Delivery method does change some side effects. Injections can cause swings. Gel may irritate skin. Pellets can bruise or get infected at the insertion site.
No option is risk-free. But when done right, TRT is generally well tolerated.
Money and routine matter more than people admit. You can pick the “best” protocol on paper and still quit if it annoys you daily.
So let’s talk real life.
Injections are usually cheapest. A few dollars per week if you pay cash. Gels cost more, especially brand names. Pellets are often the most expensive upfront but spread across months.
Convenience flips that order. Pellets win for ease. Gel comes next. Injections require the most hands-on effort.
Ask yourself simple questions. Do you travel a lot? Hate needles? Forget daily habits? Want tight dose control?
Your answers matter more than online opinions.
Testosterone Injections vs Gel vs Pellets: How to Choose Your Best Fit
By now, you’ve probably noticed something. The testosterone injections vs gel vs pellets debate isn’t about which is “best.” It’s about which you’ll actually stick with.
If you want control and low cost, injections win. For smooth levels and no needles, gel makes sense. If you want zero maintenance, pellets are appealing.
I’ll be blunt. Most people start with injections. They’re flexible and affordable. After a year, some switch once they know their body better.
And that’s okay. TRT isn’t permanent in one form. You can pivot.
Conclusion: Testosterone Injections vs Gel vs Pellets Comes Down to Your Life
So where do we land with testosterone injections vs gel vs pellets?
There isn’t a magic winner. There’s only what fits you.
If you don’t mind weekly shots and want maximum control, injections are practical and proven. It provides you with a simple daily routine and steady levels, gel feels smooth and predictable. If you crave freedom from both, pellets offer long stretches without thinking about hormones at all.
Think about your habits, budget, and tolerance for maintenance. Then choose the method you’ll actually follow. Because consistency beats perfection every time. When it comes to testosterone injections vs gel vs pellets, the best option is the one you’ll stick with for the long haul.
Because TRT isn’t about the “perfect” method. It’s about momentum.
Book the consult. Get the bloodwork. Start the protocol.
Then improve it over time.
That’s how you build energy, strength, and drive that compound for years instead of months.
Maybe your gym progress stalled or your doctor mentioned “low T” on a lab report.
And now you’re wondering if testosterone therapy is the fix.
But how does TRT work?
It’s actually simple biology.
Your body isn’t making enough testosterone, so therapy brings levels back to a healthy range. That’s it at a high level. But the details matter. Dosage, delivery method, monitoring, and expectations can make or break your results.
This guide walks you through it step by step. No fluff. No scare tactics. Just straight talk so you can decide if TRT makes sense for you.
What Testosterone Actually Does in Your Body (And Why Levels Matter)
Before you can answer how does TRT work, you need to understand what testosterone does in the first place. This hormone isn’t just about muscle or libido like most ads suggest. It helps regulate mood, bone density, red blood cell production, fat storage, and even how sharp your brain feels. When levels drop, the whole system slows down like a phone stuck in low-power mode.
Think of testosterone as a volume knob. Too low and everything feels muted. Energy dips, workouts drag, sleep suffers, and motivation fades. You might still function, but you’re not operating at full strength. That’s why doctors don’t treat symptoms alone. They look at labs and how you feel together.
If you want a deeper look at the science of low levels and age ranges, check out Normal Testosterone Levels by Age. Seeing numbers in context helps you know whether you’re truly low or just tired.
Research from The National Institutes of Health, also shows how broad testosterone’s role really is. It’s not just a “men’s hormone.” It’s a whole-body regulator.
So when someone asks how does TRT work, the real answer starts here. You’re not chasing a cosmetic boost. You’re restoring a basic biological signal your body depends on every day.
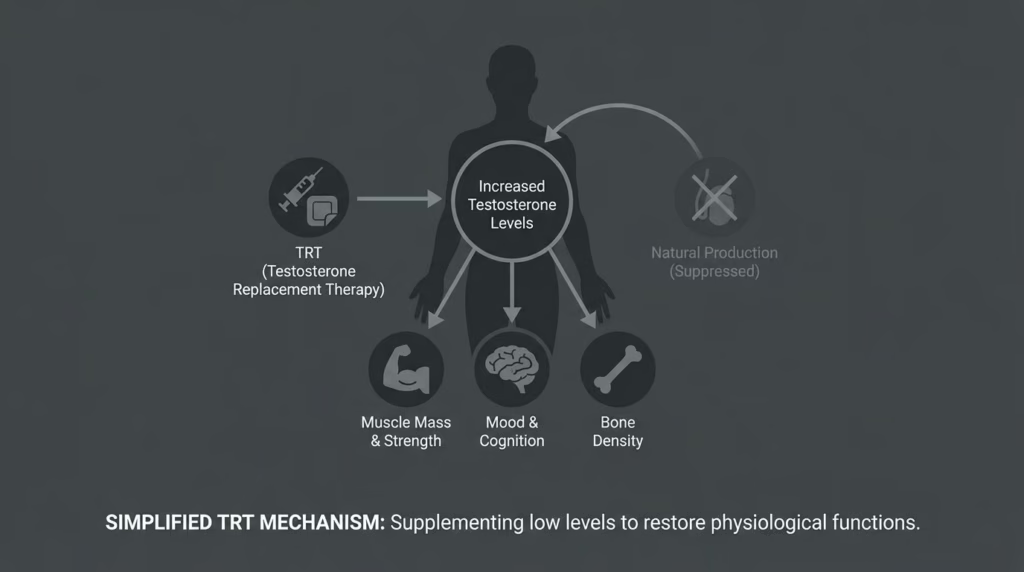
How Does TRT Work Inside Your Body? The Simple Mechanism
Let’s break it down without the medical jargon. How does TRT work at the most basic level? You replace the testosterone your body isn’t making enough of. That added hormone enters your bloodstream, binds to receptors in your cells, and tells your tissues to behave like they did when levels were normal.
Once testosterone hits those receptors, things start changing quietly. Muscle protein synthesis improves. Fat metabolism picks up. Your brain gets stronger neurotransmitter support. Red blood cell production increases. It’s not magic. It’s chemistry doing what it’s supposed to do.
Here’s the catch people miss: your body also notices the extra hormone and may reduce its own production. That’s why medical supervision matters. Dosing too high or too fast can throw off your natural feedback loops. This isn’t a “more is better” situation. It’s about balance.
If you’re brand new to the topic, you might want to start with the Complete Guide to TRT. It lays out expectations so you don’t fall for internet myths.
Who Is TRT Actually For? Signs You Might Be a Candidate
Not everyone who feels tired needs therapy. Coffee exists for a reason. But there’s a difference between “had a bad week” tired and “something’s wrong” tired. If you’re constantly drained, losing strength despite training, gaining belly fat out of nowhere, or dealing with low libido and brain fog, it’s worth asking how does TRT work for someone like you.
Doctors usually look for both symptoms and blood tests. Two separate morning labs showing low testosterone is standard. One low reading alone doesn’t mean much. Sleep, stress, or illness can temporarily tank numbers.
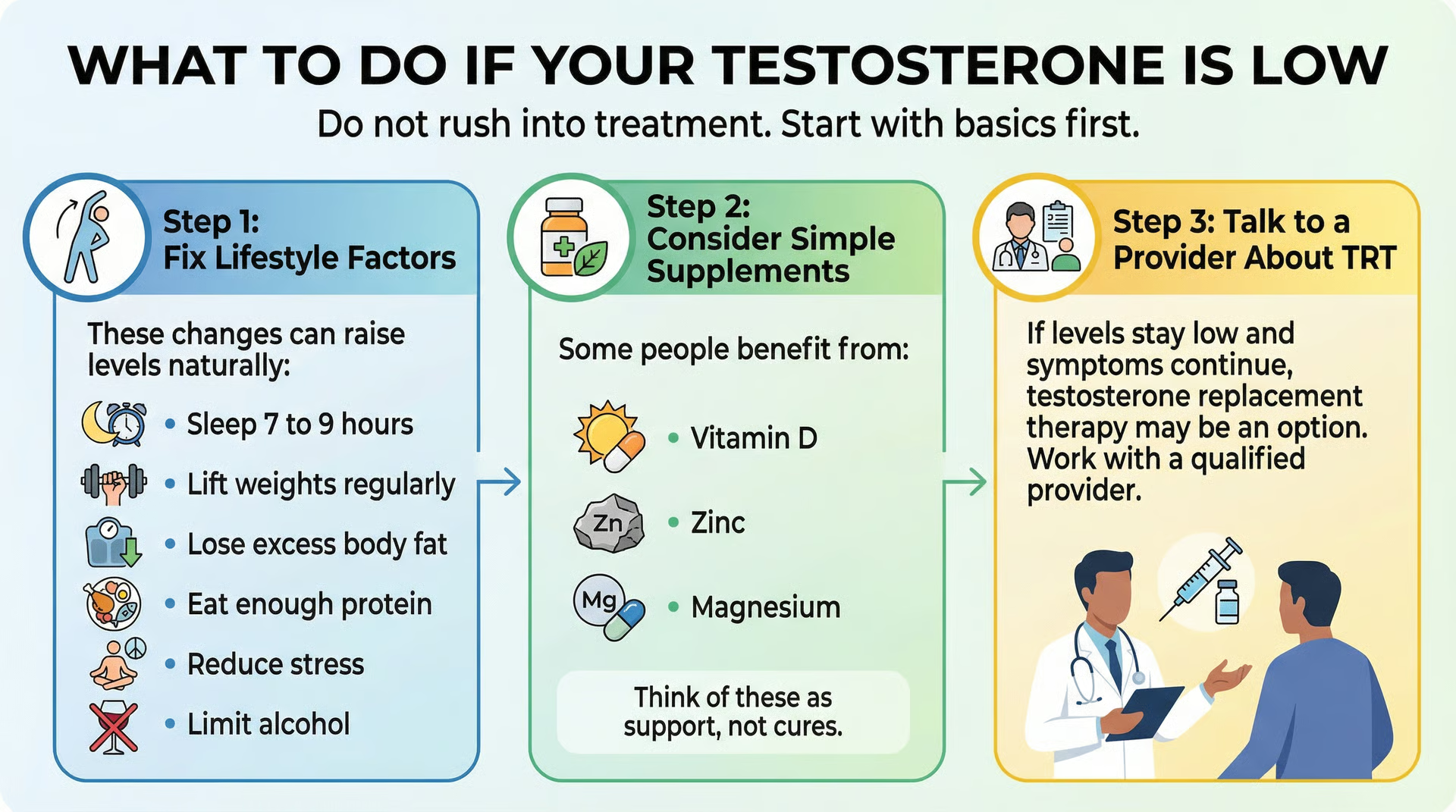
Lifestyle still comes first. Sleep more. Lift weights. Eat protein. Lose excess fat. You’d be surprised how many people fix mild issues naturally.
At that point, asking how does TRT work stops being theoretical. It becomes personal. And that’s when a real evaluation matters.
The Different Types of TRT: Injections, Gels, and More
Once you understand how does TRT work, the next question is how you’ll actually take it. There isn’t just one method. Each option delivers testosterone differently, and each has pros and cons.
Injections
Shots are the most common and often the most affordable. You inject once or twice a week, levels rise, then slowly taper until the next dose. Many people like the control and steady results.
Gels and creams
Topicals absorb through the skin daily. They’re easy but can transfer to partners or kids if you’re careless. Consistency matters. Miss a day and levels dip fast.
Pellets and patches
Pellets last months but require a small procedure. Patches are simple but can irritate skin. Fewer people use them, but they’re options.
None of these change how does TRT work biologically. They just change delivery speed and convenience. Your doctor helps you pick based on lifestyle and budget.
What Changes to Expect (And What Not to Expect)
Let’s be honest. Some marketing makes TRT sound like a superhero serum. It’s not. How does TRT work in real life? Gradually. Quietly. Over months.
In the first few weeks, many people notice better sleep and mood. Libido often improves early too. Around months two to three, strength and recovery start climbing. Body composition changes take longer, especially if diet and training aren’t dialed in. TRT supports effort. It doesn’t replace it.
What doesn’t happen? You don’t wake up shredded. You don’t gain twenty pounds of muscle without lifting. And you don’t feel euphoric 24/7. Anyone promising that is selling fantasy.
If you’re focused on maximizing results, it is important to build a nutrition plan that can help you match your hormones with smart eating.
So again, how does TRT work? It creates the conditions for normal function. You still have to show up and do the work.
Safety, Side Effects, and Monitoring
This section matters more than any sales pitch. How does TRT work safely? With monitoring. Period.
Testosterone can raise red blood cells, affect cholesterol, and suppress natural production. None of these are automatically dangerous, but they need tracking. Good clinics run labs every few months and adjust doses. Bad ones just refill prescriptions and hope for the best. Don’t trust the second group.
Common side effects can include acne, fluid retention, or mood swings when doses are too high. Fertility can also drop because your body slows its own sperm production. If kids are in your future, say that upfront. There are ways to protect fertility.
When someone casually asks how does TRT work, they often ignore this safety piece. But long-term success depends on labs, communication, and realistic dosing. Treat it like healthcare, not a shortcut.
Cost, Commitment, and Long-Term Thinking
Here’s the uncomfortable truth. Starting therapy isn’t like taking a short course of antibiotics. How does TRT work long term? It works as long as you’re on it. Stop, and levels usually fall back to baseline.
That means cost matters. Medication, labs, and appointments add up. Some insurance plans help. Others don’t. Budget realistically so you’re not forced to quit halfway through.
It’s also a lifestyle decision. Weekly injections. Routine labs. Paying attention to sleep and training. For many people it’s worth it, but you should go in clear-eyed.
Personally, I think TRT makes sense when symptoms are real and numbers confirm it. But chasing it because a podcast said “optimize everything”? That’s shaky logic. Ask yourself why you want it.
When you understand how does TRT work, you realize it’s maintenance, not a quick fix. And maintenance requires commitment.
Conclusion: So, How Does TRT Work and Is It Right for You?
By now you’ve seen the big picture. How does TRT work? It replaces missing testosterone, restores normal signaling, and helps your body function the way it used to. It’s steady, predictable biology, not a miracle. When paired with training, sleep, and smart nutrition, it can feel life-changing. When used carelessly, it’s just another hassle.
If symptoms and labs both point to low levels, talk with a qualified provider and get real data. If your numbers are fine, focus on lifestyle first. Either way, knowledge beats guesswork. The more you understand how does TRT work, the easier it is to make a decision you won’t regret six months from now.
Here’s the deal. You can keep feeling like garbage and wondering “what if,” or you can get your levels checked and actually do something about it. Limitless Alternative Medicine makes it stupid simple — labs, consult, treatment plan, done. No waiting rooms. No BS. Go to limitlessaltmed.com and book a free consultation. Worst case, you find out you’re fine. Best case, you get your life back.
Complex health issues, insurance users, hands-on preference
Monthly Cost
$99–$250 (all-inclusive)
$150–$500+ (varies by billing)
Speed to Start
2–3 weeks
1–3 months
Lab Work
Local draw or at-home kit
On-site or local lab
Insurance
Rarely accepted
Often accepted
Physical Exams
Video-only
Full in-person exam
An online TRT clinic wins on convenience and cost predictability. In-person care wins on hands-on exams and insurance coverage. The best choice depends on your health complexity, budget, and lifestyle.
What Is an Online TRT Clinic? How It Works
An online TRT clinic delivers testosterone replacement therapy through telehealth instead of a physical office. You handle consultations via video call, get lab orders sent to a local testing center (or use an at-home kit), and have prescriptions shipped directly to your door.
Here’s the typical process:
Online intake — Answer questions about symptoms like fatigue, low libido, brain fog, or stubborn weight gain
Lab work — Complete bloodwork at a local lab or with an at-home collection kit
Provider review — A licensed physician reviews your results and symptoms
Treatment plan — If you qualify, you receive a personalized TRT protocol
Medication delivery — Testosterone and supplies ship to your home monthly
The convenience factor is the main draw. For men juggling careers, families, and packed schedules, an online TRT clinic removes the friction of office visits, waiting rooms, and pharmacy trips.
But convenience alone isn’t everything. The quality of care matters just as much—and that varies significantly between providers.
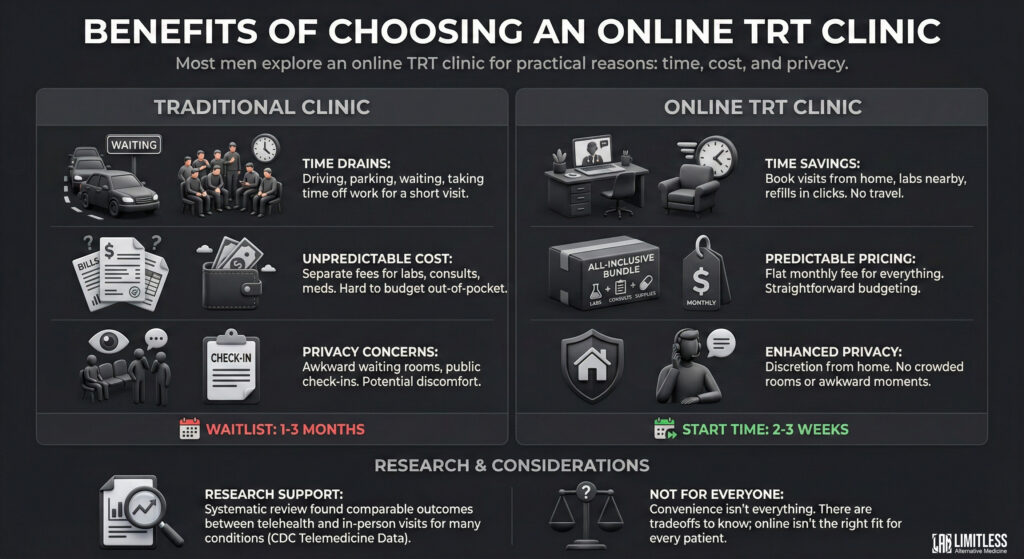
Most men explore an online TRT clinic for practical reasons: time, cost, and privacy.
Time Savings
Traditional clinics require driving, parking, waiting, and often taking time off work—all for a 10-minute conversation. An online TRT clinic eliminates that. You book visits from home, complete labs at a nearby facility, and handle refills with a few clicks.
Predictable Pricing
Many telehealth TRT providers bundle everything—labs, consultations, medications, and supplies—into a flat monthly fee. That makes budgeting straightforward, especially if you’re paying out of pocket.
Privacy
Some men feel uncomfortable discussing low testosterone in a crowded waiting room. Telehealth offers discretion. You talk to your provider from home with no awkward check-in moments.
Faster Start Times
Most online services initiate treatment within two to three weeks. Local endocrinologists and urologists often have waitlists stretching one to three months. When you’re exhausted and foggy every day, that difference matters.
Research continues to support the effectiveness of virtual care for appropriate patients. A systematic review published during the pandemic found comparable outcomes between telehealth and in-person visits for many conditions (CDC Telemedicine Data).
Still, an online TRT clinic isn’t the right fit for everyone.
Still, convenience isn’t everything. There are tradeoffs you need to know.
When In-Person TRT Visits Make More Sense
Telehealth works well for straightforward cases. But sometimes face-to-face care is the smarter move.
Complex Health Histories
If you have cardiovascular disease, diabetes, sleep apnea, or a history of prostate issues, in-person evaluation adds a layer of safety. Physical exams catch things video calls can’t—blood pressure readings, body composition changes, and other clinical signs.
Preference for Human Connection
Some men simply trust in-person conversations more. That rapport with a physician you can shake hands with matters to them. If that’s you, honor it.
Accountability
When you physically show up to appointments, you’re less likely to skip labs or delay follow-ups. With an online TRT clinic, it’s easy to procrastinate. “I’ll schedule labs next week” becomes three months.
Insurance Coverage
Many brick-and-mortar clinics accept insurance. Most online TRT services operate on a cash-pay model. If your coverage is solid, in-person care might actually cost less long-term.
If you want to know how insurance fits into TRT costs, check this breakdown: Does Insurance Cover TRT
Initial consultation, blood work, unlimited support, customized prescription, all follow-up appointments and labs Fin vs Fin
—
Premium concierge experience; any dosage
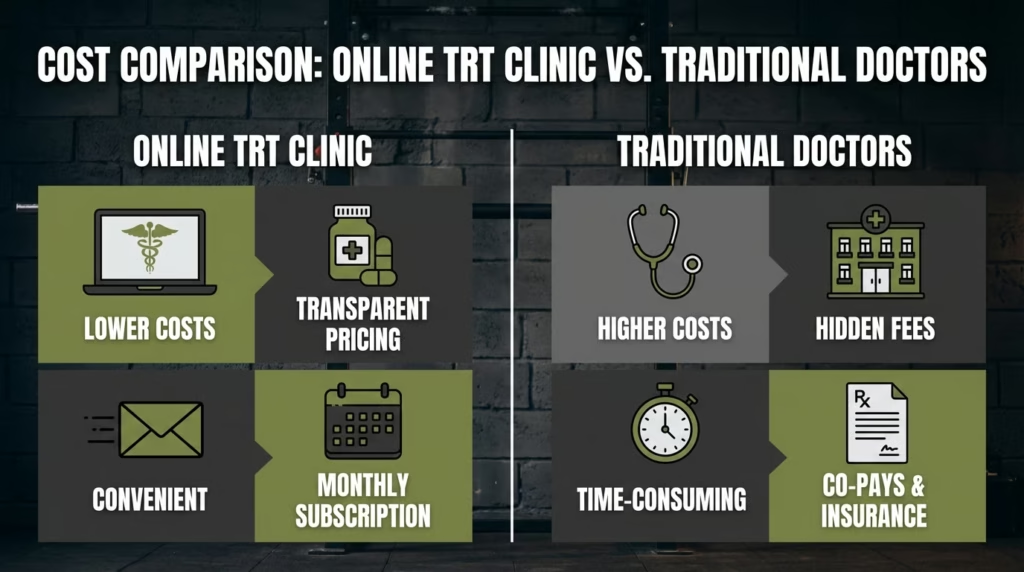
Most online TRT clinics charge $99 to $250 per month depending on medication type, dosing, and included services.
Traditional In-Person Costs
In-person clinics typically bill separately:
Initial consultation: $150–$300
Lab work: $100–$400 (depending on panel)
Follow-up visits: $75–$200 each
Medication: $40–$200/month (varies by pharmacy and type)
One month might cost $90 with insurance. The next might hit $400 if labs are due.
The Real Comparison
If you’re self-paying: An online TRT clinic usually wins. Bundled pricing removes surprises.
If insurance covers most costs: Traditional clinics can be surprisingly affordable. Run the math on your specific plan.
Watch for hidden fees: Some online services charge extra for needles, shipping, “premium support,” or specific medications. Read the fine print.
Is an Online TRT Clinic Safe? Monitoring & Quality
This is the part that matters most. Testosterone therapy changes your hormones. That means proper monitoring is non-negotiable.
What Good Monitoring Looks Like
A responsible online TRT clinic should order labs:
Before treatment — Baseline total testosterone, free testosterone, estradiol, hematocrit, PSA, lipid panel, liver enzymes, metabolic panel
6–8 weeks after starting — To assess response and adjust dosing
Every 3–6 months ongoing — To ensure safety and optimize levels
Lab Markers to Track
Marker
Why It Matters
Total Testosterone
Primary measure of therapy effectiveness
Free Testosterone
The usable, unbound portion
Hematocrit
TRT can thicken blood; elevated levels increase clot risk
Estradiol (E2)
Testosterone converts to estrogen; imbalances cause side effects
PSA
Monitors prostate health
Lipid Panel
TRT can affect cholesterol
Liver Enzymes
Monitors metabolic health
Red Flags to Avoid
If any online TRT clinic does the following, walk away:
Prescribes testosterone without lab work
Doesn’t require follow-up labs after starting
Has no licensed physicians on staff (only “coaches”)
Won’t let you speak directly with a clinician
Pushes unnecessarily high doses
A quality telehealth provider can be just as thorough as an in-person clinic. But not all platforms are equal. Some are essentially prescription mills. That’s risky.
An online trt clinic can be just as safe as in-person care. But only if it’s run responsibly.
Normal Testosterone Levels by Age
Understanding where your levels fall helps you evaluate whether treatment makes sense.
Total Testosterone Reference Ranges (ng/dL)
Age
Normal Range
Low T Cutoff
20–24
409–558
Below 409
25–29
413–575
Below 413
30–34
359–498
Below 359
35–39
352–478
Below 352
40–44
350–473
Below 350
45+
300–600 (varies)
Below 300
Source: Journal of Urology (2022), American Urological Association
The traditional 300 ng/dL cutoff was developed from studies of older men. Research now shows younger men have higher normal ranges—and may experience symptoms even when technically “in range.”
Many men start noticing low T symptoms when levels drop into the 400s, even though that’s technically “normal.”
Choosing Based on Your Lifestyle
Here’s where things get personal.
Choose an Online TRT Clinic If You:
Travel frequently for work
Hate waiting rooms and prefer texting over phone calls
Want predictable monthly costs
Value privacy and discretion
Have a straightforward health history
Choose In-Person Care If You:
Have complex health conditions requiring physical exams
Prefer face-to-face accountability
Have good insurance coverage
Want access to additional services (ultrasound, comprehensive panels)
Stick to routines better with scheduled office visits
The Hybrid Approach
Some men use both. They manage prescriptions through an online TRT clinic for convenience but see a local urologist or endocrinologist annually for comprehensive exams. That combination can offer the best of both worlds.
Think about your real behavior—not your ideal behavior. Choose the setup you’ll actually stick with.
How to Choose the Right Online TRT Clinic
If telehealth is your move, don’t just pick the first ad you see.
Evaluation Checklist
✅ Licensed physicians — Not just “health coaches” or nurse practitioners working independently ✅ Comprehensive lab panels — At least 8–10 markers before treatment ✅ Clear follow-up protocol — Labs at 6–8 weeks, then every 3–6 months ✅ Direct clinician access — Can you message or call your provider? ✅ Transparent pricing — No hidden fees for supplies, shipping, or consultations ✅ Personalized dosing — Protocols adjusted based on your labs and symptoms ✅ Positive reviews — Look for mentions of follow-up care, not just fast shipping
Questions to Ask Before Signing Up
Are there any additional costs beyond the monthly fee?
How often will I have lab work done?
Who reviews my labs—a physician or someone else?
Can I message my provider directly between appointments?
A solid online trt clinic should feel like healthcare, not a supplement store. If it feels sketchy, trust your gut.
Online TRT Clinic Red Flags: What to Avoid
Not every telehealth provider operates responsibly. Here’s what should make you pause:
Red Flag
Why It’s a Problem
No lab work required
Can’t safely prescribe without baseline data
“One-size-fits-all” dosing
TRT requires individualized protocols
No follow-up labs scheduled
Impossible to monitor safety or effectiveness
Only “coaches” available
You need licensed physicians making medical decisions
Pressure tactics or urgency
Legitimate providers don’t rush you
Unusually low prices
May indicate corner-cutting on care quality
No clear refund or cancellation policy
Sign of poor business practices
Frequently Asked Questions
Is an online TRT clinic legitimate?
Yes, when properly run. Legitimate online TRT clinics employ licensed physicians, require comprehensive lab work before prescribing, and monitor patients with regular follow-up testing. Look for providers with transparent protocols and real physician oversight—not just coaches reading scripts.
How much does an online TRT clinic cost per month?
Most online TRT clinics charge between $99 and $250 per month. This typically includes consultations, lab coordination, and medication. Some providers bundle everything; others charge separately for labs or specific medications. Traditional in-person care may cost more or less depending on insurance coverage.
Can I get TRT without seeing a doctor in person?
Yes. Federal telehealth regulations allow qualified physicians to prescribe testosterone after a virtual consultation and lab review. You’ll complete bloodwork at a local lab or with an at-home kit, then consult via video call. Most states permit this model, though regulations vary.
How fast can I start TRT through an online clinic?
Most patients begin treatment within two to three weeks of their initial consultation. This includes time for lab work and provider review. Traditional specialists often have waitlists of one to three months.
Do online TRT clinics accept insurance?
Most do not. The majority operate on a cash-pay model with transparent monthly pricing. However, you may be able to submit claims for out-of-network reimbursement depending on your plan. Some providers like OnMen (Canada) offer insurance integration.
What labs are required before starting TRT?
A responsible provider will order: total testosterone, free testosterone, estradiol, hematocrit, PSA, complete metabolic panel, lipid panel, and liver enzymes at minimum. Some clinics test 40+ markers for a more complete picture.
Is online TRT as safe as in-person treatment?
When properly monitored, yes. Safety depends on protocol quality—not location. The key factors are comprehensive baseline labs, regular follow-up testing, and responsive clinician oversight. A good online TRT clinic can provide all of these.
Final Verdict: Online TRT Clinic or In-Person?
If you want the short version:
An online TRT clinic usually wins on convenience, speed, and predictable costs. It’s ideal for men with straightforward health profiles who value flexibility and privacy.
In-person care often wins on hands-on exams, insurance coverage, and face-to-face trust. It’s better for men with complex health histories or those who prefer traditional medical relationships.
Neither option is perfect. Neither is wrong.
What matters most is consistent labs, responsible dosing, and a provider who actually listens. That can happen through a screen or across a desk.
Choose the setup you’ll actually follow through with. Because the best testosterone treatment plan is the one you’ll keep.
Want the convenience of online TRT with real clinical oversight? Limitless Alternative Medicine offers virtual consultations, at-home lab kits, and personalized protocols — all from providers who actually listen. [Book your free consultation] and see if TRT is right for you.
TL;DR Telemedicine weight loss blends medical care with the ease of virtual access. For a lot of people, that mix finally makes consistency possible. Licensed providers, individualized plans, and regular check-ins remove many of the friction points that usually knock progress off track. If clinic visits are where things always fall apart, this model is worth a serious look.
What Telemedicine Weight Loss Really Is
There’s still confusion here.
Telemedicine weight loss isn’t a calorie-counting app or a generic PDF meal plan.
It’s medical care, delivered remotely.
Licensed clinicians. Real evaluations. And prescriptions, when they make sense.
That difference matters more than most people realize.
Programs usually start with a thorough intake. Medical history. Current medications.
Lifestyle habits that don’t show up on a scale. Some providers send patients for labs locally. Others rely on validated screenings. From there, the plan gets built around the person, not a template pretending to be “custom.”
What it isn’t is fast. And it isn’t effortless. No responsible provider claims that. Weight didn’t build overnight, and it doesn’t disappear that way either. Programs promising “no work” results usually don’t last long.
Where telemedicine weight loss stands out is in sustainability. The focus isn’t on dramatic drops. It’s creating something people can actually live with.
If you’re curious how this compares with traditional clinics, this breakdown helps:
How virtual care compares to in-person weight loss clinics
How Virtual Medical Support Changes the Weight Loss Game
Most people don’t struggle because they don’t know what to eat. They struggle because no one notices when things stall. Or when side effects creep in. Or when motivation fades quietly.
That’s where virtual medical support earns its place.
Regular check-ins mean plateaus don’t drag on for months. Adjustments happen sooner. Patterns get noticed. When something stops working, it gets addressed instead of ignored. That alone prevents a lot of silent quitting.
Convenience matters more than people like to admit. No traffic. No waiting rooms. No burning half a day for a short appointment. When care fits into real life, follow-through improves. And consistency more than intensity is what actually moves the needle.
Access matters too. Rural patients. Busy professionals. Parents juggling schedules. Telemedicine opens doors that used to stay shut. Broader healthcare data shows better follow-up and adherence with virtual care.
If accountability has always been your weak spot, this explains why timing and support matter more than raw motivation.
The Role of Prescription Medications In It
This is where confusion piles up.
Yes, some telemedicine weight loss programs use medication. No, that doesn’t mean everyone gets it. And it’s not a shortcut.
Medications like GLP-1 agonists or appetite regulators are tools. Useful ones, but only when paired with guidance and monitoring. A responsible provider doesn’t hand over a prescription and disappear.
Virtual monitoring lets clinicians track progress, manage side effects, and adjust doses. Sometimes medication gets paused. Sometimes it’s stopped altogether. That ongoing relationship often makes the difference between steady progress and frustration.
If you’re unsure whether medication belongs in your plan, understanding how providers decide eligibility clears up a lot of expectations.
Nutrition and Behavior Coaching Still the Backbone
Medication gets attention. Coaching does most of the work.
The difference with telemedicine weight loss is how coaching shows up. It’s not a one-time lecture. It’s ongoing and practical, built around real life, travel weeks, stress spikes, late dinners, and social pressure.
Virtual platforms often include messaging, food tracking, and regular reviews. That steady feedback loop builds awareness without turning meals into math problems. Most people are also more honest remotely. Less performative. Fewer half-truths.
Behavior research backs this up. Consistent coaching improves long-term maintenance, especially with medical oversight.
This research shows that maintaining behavior change, not just starting it, is what drives long-term success.
Telemedicine weight loss fits especially well for busy parents, remote workers, frequent travelers, and anyone burned out on scheduling appointments. It also works well for people who feel uncomfortable in traditional clinic settings.
It isn’t perfect for everyone. Patients with complex medical issues may still need in-person care alongside virtual support. Good programs are upfront about that. If someone claims virtual care works for everyone, that’s usually a warning sign.
Age and location aren’t the real limits. Engagement is. When patients stay involved and communicate honestly, results tend to follow.
Cost matters too. Many people find virtual programs cheaper over time because missed visits and unnecessary appointments drop. Knowing the pricing upfront avoids a lot of frustration.
Common Myths That Still Need to Die
One myth that won’t go away: telemedicine weight loss isn’t “real” medicine. Licensed clinicians don’t lose their training through a screen.
Another is that it’s only for people with a little weight to lose. Many programs treat obesity as the chronic condition it is, with long-term strategies instead of quick fixes.
Then there’s the idea that virtual care feels distant. In practice, many patients say the opposite. Having message access alone changes how supported people feel between visits.
And no, it’s not cheating. Using medical support to improve health is practical. If long-term success matters to you, this analysis adds a useful perspective.
Choosing the Right Telemedicine Weight Loss Program
The platform matters less than the people running it.
You should know who your provider is, what their credentials are, and how follow-ups work. Vague answers now usually mean problems later.
Be cautious with programs that promise exact timelines or hide pricing. Weight loss is personal. Predicting it like clockwork isn’t realistic.
Reviews help, but patterns matter more than perfection. Look for steady feedback about communication, responsiveness, and support, not just dramatic before-and-after photos.
Knowing what to ask before enrolling saves time and stress.
The Emotional Side of Weight Loss That Telemedicine Actually Addresses
This part rarely gets enough attention.
Weight loss carries emotional weight, frustration, shame, and burnout. Traditional settings sometimes make it heavier. Virtual care often lowers the pressure.
From home, people open up more. They admit when they’re struggling. They ask the questions they usually keep to themselves. That honesty leads to better adjustments and fewer silent dropouts.
Frequent check-ins matter. A short message at the right moment can stop a spiral. Weight loss usually doesn’t fail because of one meal. It fails because people feel alone afterward.
Support changes behavior. Quietly, but steadily.
Why Consistency Becomes Easier With It
Consistency isn’t exciting. It’s just effective.
Telemedicine weight loss removes many of the barriers that wreck it. Appointments fit into lunch breaks. Adjustments happen quickly. Problems don’t sit unresolved for months.
Small touchpoints add up. Weekly check-ins. Small course corrections. That responsiveness keeps momentum alive.
Plateaus feel less threatening when someone helps interpret them. Stress, sleep, hormones, often, the fix isn’t extreme. It’s specific.
How It Plays Out for Busy Lives (Because Life Doesn’t Pause)
Most people don’t quit because they stop caring. They quit because life gets messy.
Virtual care adapts. Travel weeks lead to nutrition tweaks. Stress spikes trigger behavioral support. Missed workouts mean recalibration, not guilt.
That flexibility keeps plans alive when life gets complicated. And since life always gets complicated, that matters.
What Long-Term Success Looks Like in Telemedicine Weight Loss
Fast drops look impressive. They aren’t the whole story.
Long-term success means learning patterns, hunger cues, stress responses, and habit loops. Telemedicine weight loss supports that learning over time.
As progress stabilizes, responsibility slowly shifts back to the patient. Not suddenly. That gradual handoff builds confidence instead of dependence.
Maintenance planning is often where outcomes are decided. Programs that talk about it early tend to do better.
It Isn’t a Trend It’s a Shift
Some still think telemedicine weight loss with GLP-1 is temporary. It isn’t.
Healthcare is moving toward access and continuity. Virtual care fits naturally there. Patients want support that works with their lives, not against them.
Clinics won’t disappear. But care is becoming more flexible. More responsive. More realistic.
Why the Right Mindset Still Matters
Even the best tools don’t replace effort.
Telemedicine weight loss works best as a partnership. Logging meals. Showing up for check-ins. Being honest. When patients engage, outcomes improve.
The difference is that virtual care makes those things easier. Asking for help feels simpler. Feedback comes faster. Progress feels possible.
Weight loss doesn’t have to feel punishing. With the right support, it usually feels manageable.
FAQs
Is telemedicine weight loss safe?
Yes, when it’s run by legitimate providers who follow medical guidelines and monitor patients over time.
Do I have to take medication?
No. Medication is optional and only used when it makes medical sense.
How fast will I see results?
It varies. The goal is steady, sustainable progress, not dramatic drops.
Can it replace in-person visits?
For many people, yes. Some conditions still need in-person care.
Is it covered by insurance?
That depends on your plan. Some programs offer reimbursement or HSA/FSA options.
Let’s Summarize It
Telemedicine weight loss works because it lines up with real life. Medical oversight, convenience, and accountability come together in ways traditional programs often struggle to match.
It isn’t effortless. But it is realistic. And that realism is why people stick with it.
If you’ve been stuck, restarting, or tired of doing this alone, this approach might fill the gap, not because it’s trendy, but because it treats weight loss as the complicated medical and behavioral process it really is.
Want To Start Seeing Results?
If restarting every few months feels familiar, it might be time for a different approach. Telemedicine weight loss offers structure, support, and flexibility without constant clinic visits. Progress shouldn’t depend on willpower alone. Connect with a provider who supports you between appointments and build something that actually lasts.
Why TRT Blood Test Requirements Matter for Safe Treatment
TRT blood test requirements exist because low testosterone shares symptoms with about two dozen other conditions. Depression. Thyroid dysfunction. Sleep apnea. Diabetes. They all do a very convincing impression of low T. Without proper bloodwork, your provider would essentially be guessing.
There’s also a safety component that doesn’t get talked about enough. Reputable clinics won’t touch you without baseline labs because they need to know where you started. If six months down the road your red blood cell count spikes or your liver enzymes go haywire, they need that original data to compare against. It protects you. It protects them. It’s the boring, responsible thing that makes all the exciting stuff possible later.
The Endocrine Society’s Clinical Practice Guideline on Testosterone Therapy (the closest thing this field has to a bible) specifically recommends that hypogonadism should only be diagnosed in men who have both symptoms consistent with testosterone deficiency and consistently low serum testosterone confirmed on at least two separate morning draws. Two. Not one. Because even your hormones have bad days.
Complete TRT Blood Test Panel: Every Lab You Need
Here’s a quick-reference summary of every test in a full TRT blood test panel, followed by a detailed breakdown of what each one tells your doctor.
TRT Blood Test Requirements: Summary Table
Test
What It Measures
Why It Matters for TRT
Total Testosterone
All testosterone (bound + free)
Determines if levels are clinically low
Free Testosterone
Unbound, usable testosterone
Often low even when total T is “normal”
SHBG
Protein that binds testosterone
Explains the gap between total and free T
Estradiol (E2)
Primary male estrogen
Baseline needed to manage aromatization on TRT
CBC (Complete Blood Count)
Red/white blood cells, hematocrit
TRT raises hematocrit — must monitor for clot risk
CMP (Comprehensive Metabolic Panel)
Liver, kidney, blood sugar, electrolytes
Confirms organs can safely process exogenous testosterone
Lipid Panel
Cholesterol and triglycerides
TRT can shift lipid profiles in either direction
PSA (Prostate-Specific Antigen)
Prostate health marker
Baseline needed to monitor prostate during treatment
LH & FSH
Pituitary signaling hormones
Distinguishes primary from secondary hypogonadism
Thyroid Panel (TSH, Free T3, Free T4)
Thyroid function
Rules out thyroid dysfunction mimicking low T
Prolactin
Pituitary hormone
Elevated levels suppress testosterone; may indicate adenoma
Vitamin D
Vitamin D status
Deficiency linked to lower testosterone production
Ferritin
Iron storage
Low iron causes fatigue often mistaken for low T
Total Testosterone and Free Testosterone: The Core TRT Blood Tests
Total Testosterone is the headliner. This measures all the testosterone in your bloodstream, both the stuff bound to proteins and the stuff floating free. Most labs call anything between 300–1,000 ng/dL “normal,” but there’s an enormous, contentious, surprisingly emotional debate about what “normal” even means. A 35-year-old sitting at 310 ng/dL is technically in range. He’s also probably feeling like a phone at 4% battery. Context matters. A good provider looks at your number in relation to your age, your symptoms, your life. Not just whether it clears some arbitrary threshold.
Free Testosterone is, arguably, the more important number, and it’s the one a lot of providers forget. Only about 2–3% of your testosterone is actually “free,” meaning available for your body to use. The rest is bound to proteins like SHBG and albumin, just riding around doing nothing, like a guy on a bus who missed his stop and is too polite to say anything. You could have decent total testosterone and rock-bottom free T, and you’d still feel terrible. Make sure this is on your panel.
SHBG and Estradiol: The Hormones That Shape Your TRT Protocol
Sex Hormone-Binding Globulin (SHBG) is the protein that determines how much of your testosterone is free versus bound. High SHBG grabs your available testosterone and holds it hostage. Low SHBG can signal other metabolic issues. Either way, this number helps your doctor understand the full equation, not just the headline.
Estradiol (E2) is a form of estrogen, and yes, men produce it. When you start TRT, your body converts some testosterone into estradiol through a process called aromatization, which is a lovely word for something that can become not-lovely fast. Too much estradiol: water retention, mood swings, breast tissue growth. Too little: joint pain, brain fog, a general feeling of wrongness. Baseline levels help your provider calibrate treatment and decide whether you’ll need an aromatase inhibitor down the road.
Blood Health and Safety Markers Required Before Starting TRT
Here’s where we shift from “what’s your testosterone doing” to “can your body actually handle this.” These are the tests that keep you safe. They’re not glamorous. They will never be the subject of a podcast. They matter enormously.
CBC: The TRT Blood Test That Monitors Clot Risk
Complete Blood Count (CBC) matters, and here’s why: TRT stimulates red blood cell production. That’s a well-documented effect. Sounds fine, right? More red blood cells, more oxygen delivery, more vitality? Sure, up to a point. Past that point, your blood gets thicker. And thicker blood is not the win it sounds like. Thicker blood means higher risk of clots, stroke, cardiovascular events. The kind of things that make you wish you’d been more careful.
A 2022 study published in The Journal of Urology looked at data from over 74 million patients and found that men who developed secondary polycythemia (hematocrit at or above 52%) while on testosterone therapy had a 35% increased risk of major adverse cardiovascular events and venous thromboembolism in the first year of treatment. Thirty-five percent. That’s not a rounding error. That’s why your doctor needs a baseline CBC and why they’ll keep checking it.
Metabolic Panel, Lipids, and PSA: Organ Function Before TRT
Comprehensive Metabolic Panel (CMP) covers liver function, kidney function, blood sugar, and electrolytes. Your liver processes testosterone. If your liver enzymes are already elevated, if your liver is already, metaphorically, working a double shift, piling TRT on top would be reckless. Same for kidneys. These organs are doing hard, unglamorous, essential work. Your provider needs to know they’re up to the task before adding to their workload.
Lipid Panel checks cholesterol and triglycerides. Testosterone can shift your lipid profile, sometimes for the better, sometimes not. If you’ve already got borderline cholesterol, your doctor might want to address that before or alongside starting therapy. This isn’t gatekeeping. This is making sure you don’t solve one problem by creating another.
Prostate-Specific Antigen (PSA) is required for men over 40, and frankly it’s smart for anyone starting TRT. Testosterone does not cause prostate cancer. That old myth has been largely put to rest. But testosterone can accelerate existing prostate conditions, which is a meaningful distinction. A baseline PSA gives your provider a reference point for all future monitoring.
Additional TRT Blood Tests Most Clinics Skip
Here’s where you find out how good your clinic actually is. The budget operations check your total T, maybe your CBC, and call it a day. A thorough provider goes further. And you should insist on it, even if it means being the slightly annoying patient. Be the slightly annoying patient. Your health is worth a little social discomfort.
LH and FSH: Diagnosing the Cause of Low Testosterone
Luteinizing Hormone (LH) and Follicle-Stimulating Hormone (FSH) tell your doctor why your testosterone is low, which turns out to be a fairly important question. Is the problem in your testes (primary hypogonadism) or in your brain’s signaling system (secondary hypogonadism)? This distinction changes everything. Secondary hypogonadism might respond to clomiphene or hCG, potentially making TRT unnecessary altogether. Without LH and FSH testing, you’re skipping a diagnostic step that could save you years of injections.
Thyroid Panel: Ruling Out the Most Common TRT Misdiagnosis
Thyroid Panel (TSH, Free T3, Free T4) is one I feel strongly about. Thyroid dysfunction mimics low testosterone almost perfectly. Fatigue. Weight gain. Brain fog. Low libido. The overlap is uncanny. I’ve seen forum after forum full of guys who jumped on TRT when their real issue was hypothyroidism. A simple, inexpensive thyroid panel could’ve saved them months of unnecessary medication and the particular frustration of treating the wrong thing.
Prolactin: The Overlooked TRT Blood Test That Can Save Your Health
Prolactin gets overlooked with startling frequency. Elevated prolactin suppresses testosterone production and causes symptoms like low sex drive and, in some cases, breast tissue growth. Here’s the thing that makes this one urgent: high prolactin sometimes indicates a pituitary adenoma. That’s a benign brain tumor. It sounds terrifying, but it’s actually very treatable if you catch it. The Pituitary Society’s international consensus statement, published in Nature Reviews Endocrinology, notes that prolactinomas account for roughly half of all pituitary adenomas and respond remarkably well to dopamine agonist medications like cabergoline. But you have to know it’s there first. Don’t skip this test.
Vitamin D and Ferritin: Deficiencies That Mimic Low Testosterone
Vitamin D and Ferritin might seem like they wandered in from a different appointment, but they’re connected to testosterone production in ways that matter. Vitamin D deficiency is linked to lower testosterone levels. Low ferritin (your iron storage marker) causes fatigue that looks identical to low T fatigue. Sometimes correcting these deficiencies improves testosterone on its own. No injections. No protocol. Just your body working the way it wants to when you give it what it needs.
How to Prepare for Your TRT Blood Tests
You can’t roll out of bed at 3 PM, grab a large coffee, and expect your bloodwork to mean anything. How and when you get your blood drawn matters. A lot. Testosterone fluctuates throughout the day, and certain behaviors can tilt your results in directions that don’t represent reality.
Get your blood drawn in the morning. Ideally between 7 AM and 10 AM. Testosterone peaks in the early morning hours and can drop 30–40% by afternoon. Test in the evening and you might look hypogonadal on paper when you’re actually fine.
Fast for 8–12 hours beforehand. This isn’t just for the lipid panel. Eating can temporarily affect hormone levels too. Water is fine, and actually helpful (hydrated veins are cooperative veins). But skip the food, the sugary drinks, and definitely the alcohol the night before.
Sleep well the night before. This sounds like your mother talking, but she’s right. Poor sleep tanks testosterone levels temporarily. One bad night can drop your T by 10–15%. If you pulled an all-nighter or got four hours because anxiety about the appointment kept you staring at the ceiling, your results won’t reflect your real baseline.
Skip intense exercise for 24–48 hours before your test. Heavy lifting spikes testosterone temporarily, which sounds great until you realize it gives your doctor a falsely elevated reading. You want your resting baseline, the real number, not your post-deadlift peak.
Tell your doctor about everything you’re taking. Medications, supplements, all of it. Opioids and corticosteroids affect hormone levels. Biotin (which hides in a surprising number of men’s multivitamins) can actually interfere with lab assays and produce false readings. Full disclosure upfront saves everyone headaches later.
What Happens After Your TRT Blood Test Results Come Back
So you’ve done the bloodwork. You’ve waited the agonizing 3–7 days, which is enough time to convince yourself of approximately forty different diagnoses. Now you’re staring at numbers that may or may not make sense.
Your provider reviews the full panel, not just your testosterone number in isolation. They’re looking for patterns. Relationships. Stories the numbers tell when you read them together. Low total T plus low LH might point to a pituitary issue. Low free T with high SHBG tells a different story than low free T with normal SHBG. Elevated liver enzymes might mean you need additional workup before anyone talks about treatment. It’s all connected, and a good doctor treats it that way. For a deeper look at how these markers interact and why interpretation is more nuanced than simple reference ranges, the PMC review on challenges in testosterone measurement and data interpretation is an excellent resource.
Most providers will want two separate low testosterone readings before diagnosing hypogonadism. That’s not them being difficult. It’s standard medical practice. Testosterone fluctuates day to day based on stress, sleep, illness, whether you had a fight with your brother, whether the dog kept you up. A single low reading could be a fluke. Two confirms a pattern.
If your results confirm low testosterone, your provider will discuss treatment options based on your specific situation. TRT is not one-size-fits-all. Your age, fertility goals, other health conditions, and the type of hypogonadism you have all factor into the protocol they recommend. Some guys thrive on injections. Others prefer topical gels or pellets. The initial bloodwork guides that decision.
Once you start treatment, expect more bloodwork. Typically at the 6-week mark, then at 3 months, 6 months, and annually after that. Your doctor will track testosterone levels, hematocrit, PSA, liver function, and estradiol to make sure everything stays in a safe range. Ongoing monitoring is just as important as the initial TRT blood test requirements. Maybe more so.
TRT Blood Test Requirements: FAQ
What blood tests are required before starting TRT? A full TRT blood test panel includes total testosterone, free testosterone, SHBG, estradiol, CBC, comprehensive metabolic panel, lipid panel, PSA, LH, FSH, thyroid panel (TSH, Free T3, Free T4), prolactin, vitamin D, and ferritin. Some clinics only test total testosterone and CBC. That’s not thorough enough for safe treatment.
Why do I need two testosterone tests before starting TRT? Testosterone levels fluctuate from day to day based on sleep, stress, illness, and other factors. A single low reading could be an anomaly. The Endocrine Society recommends two separate morning blood draws with consistently low results before diagnosing hypogonadism and prescribing treatment.
What time of day should I get my TRT blood test? Between 7 AM and 10 AM, fasting. Testosterone peaks in the early morning and can drop 30–40% by afternoon. An evening test could show falsely low levels that don’t represent your actual baseline.
Do I need to fast before TRT blood work? Yes. Fast for 8–12 hours before your draw. This ensures accurate lipid panel and metabolic marker readings, and prevents food intake from temporarily affecting hormone levels. Water is fine and encouraged.
What testosterone level qualifies for TRT? Most guidelines use a total testosterone below 300 ng/dL as the threshold for diagnosing low testosterone, though the Endocrine Society and other organizations acknowledge that symptoms should be present alongside low lab values. A man at 310 ng/dL with real symptoms may still be a candidate depending on his free testosterone, SHBG, and overall clinical picture.
How often do I need blood tests after starting TRT? Typically at 6 weeks after starting, then at 3 months, 6 months, and annually thereafter. Your doctor will monitor testosterone levels, hematocrit, PSA, liver function, and estradiol to ensure treatment stays safe and effective.
Can TRT cause high red blood cell count? Yes. TRT stimulates red blood cell production, which can raise hematocrit levels. If hematocrit climbs above 52–54%, blood becomes thicker and the risk of blood clots, stroke, and cardiovascular events increases. This is why CBC monitoring throughout treatment is essential.
What if my testosterone is low but my doctor only checked total T? Ask for a full panel. Total testosterone alone doesn’t tell the full story. Free testosterone, SHBG, LH, FSH, and thyroid markers are all necessary to determine whether you truly have hypogonadism, what’s causing it, and what the right treatment approach is.
Final Thoughts on Meeting Your TRT Blood Test Requirements
I understand the impulse to skip ahead. When you feel lousy (truly, deeply lousy in that way where your own life starts to feel like something happening to someone else) the last thing you want is another obstacle between you and feeling better. Another appointment, another copay, another week of waiting.
But meeting your TRT blood test requirements isn’t an obstacle. It’s the opposite. It’s the thing that makes everything that comes after work. These labs confirm you actually need therapy, that your body can handle it safely, and that your provider has the data to get your protocol right. Not approximately right, but right for you, specifically, in your particular body with its particular history.
Don’t cut corners on this. Find a provider who runs full panels, not just a total testosterone check. Ask questions about every test they order. Ask questions about every result they explain. You are, after all, putting a powerful hormone into your body, into the only body you will ever have, and you deserve to go in understanding exactly where things stand.
Your TRT blood test requirements are your roadmap. They tell you where you’re starting. They help your doctor chart the course. They give you benchmarks to measure whether this whole thing is actually working. Treat them as the foundation they are, and you’ll be set up for the best possible version of what comes next.
Which, if you’re lucky and careful and willing to do the boring parts, might just be pretty good.
These problems often get blamed on aging or stress. Sometimes that’s true. Sometimes your hormones are the issue.
Testosterone affects strength, mood, focus, metabolism, and sex drive. When it drops, you feel it.
Testing is simple, fast, and affordable. Here’s how to do it step by step.
TL;DR: Quick Summary
The most accurate way to test testosterone is a morning blood test between 7 and 10 AM that checks total and free testosterone. You can test through your doctor, a walk-in lab like Quest or Labcorp, or an at-home finger-prick kit. Sleep well, avoid hard workouts and alcohol the day before, and test early in the day. If results are low, repeat the test to confirm before starting treatment.
We use cookies to ensure that we give you the best experience on our website. If you continue to use this site we will assume that you are happy with it.