

If you’re over 45 and have been feeling off lately:
You might have low testosterone.
About 4 to 5 million men in the United States do.
Only about 5% of them are getting treatment for it. Which means there are a lot of guys out there running on fumes, thinking this is just what getting older feels like, when in fact there’s a well-studied, medically supervised treatment that could help.
What Is TRT (and Who Is It For)?
Let’s be clear TRT is not steroids for guys who want bigger arms. It’s not simply a performance enhancer.
What it is: a medically supervised treatment that restores your testosterone to normal levels when your body has stopped producing enough on its own. Think of it less like upgrading your engine and more like putting the correct grade of oil back in it. Your car was designed to run on this stuff. Without it, things get clunky.
Clinically, your doctor will consider TRT when your total testosterone consistently falls below 300 ng/dL, the threshold recognized by the American Urological Association and the Endocrine Society, and you’re experiencing symptoms that genuinely affect your quality of life. Both pieces matter. A low number without symptoms, or symptoms without a low number, typically won’t (and shouldn’t) result in a prescription.
The Signs Something Might Be Off
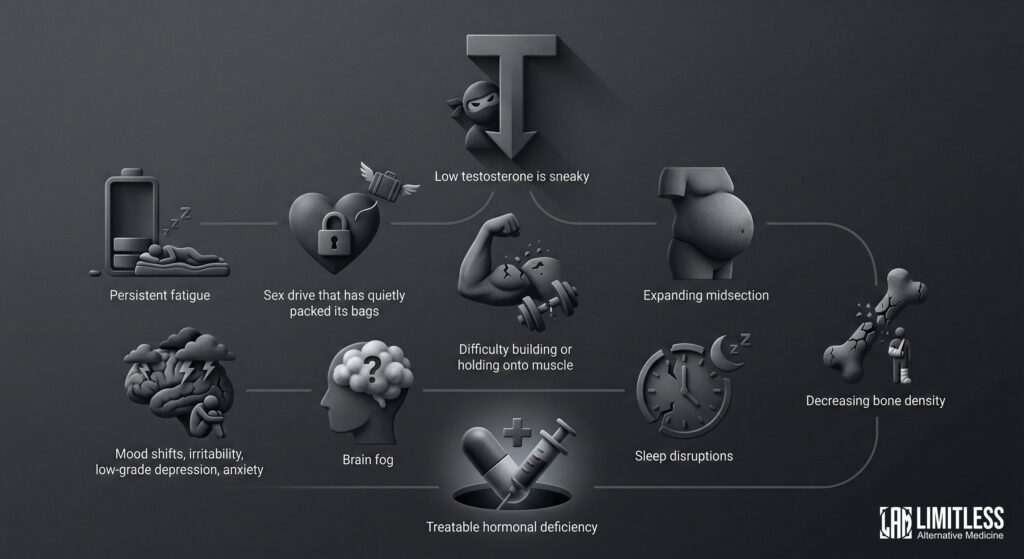
Low testosterone is sneaky. It doesn’t arrive with a banner and a trumpet.
It shows up gradually, like a guest who keeps dimming the lights at your party until suddenly you’re all sitting in the dark wondering what happened to the vibe.
The most common signs include persistent fatigue that doesn’t improve no matter how much you rest, a sex drive that has quietly packed its bags and moved to a different zip code, difficulty building or holding onto muscle even though you’re still putting in the work, an expanding midsection that seems to have its own agenda, mood shifts, irritability, a low-grade depression, anxiety that wasn’t there before, brain fog that makes you feel like you’re thinking through wet cotton, sleep disruptions, and decreasing bone density (which you won’t notice until something breaks, which is the worst way to notice).
Here’s what’s important: a lot of men chalk this up to stress, or age, or not sleeping well, or the general condition of being alive in the modern era.
And sometimes those things are the cause.
But sometimes they’re just masking a hormonal deficiency that’s entirely treatable.
The only way to know is to get tested, which we’ll get to. Or if you want a more in depth guide see: Signs of Low Testosterone in Men: What’s Really Going On.
Normal Testosterone Levels by Age
Your testosterone peaks sometime in your late teens to early twenties—back when you had opinions about everything and the energy to argue about them—and then declines about 1% per year after 30. Here’s a rough reference range for total testosterone:
| Age Range | Typical Total Testosterone (ng/dL) |
| 18–25 | 400–700 |
| 26–35 | 350–650 |
| 36–45 | 300–600 |
| 46–55 | 250–550 |
| 55+ | 200–500 |
These ranges vary by lab. What matters clinically is where your number sits relative to how you feel. A guy at 310 with zero symptoms is in a very different situation than a guy at 310 who can barely get through his afternoon without a nap and a small existential crisis.
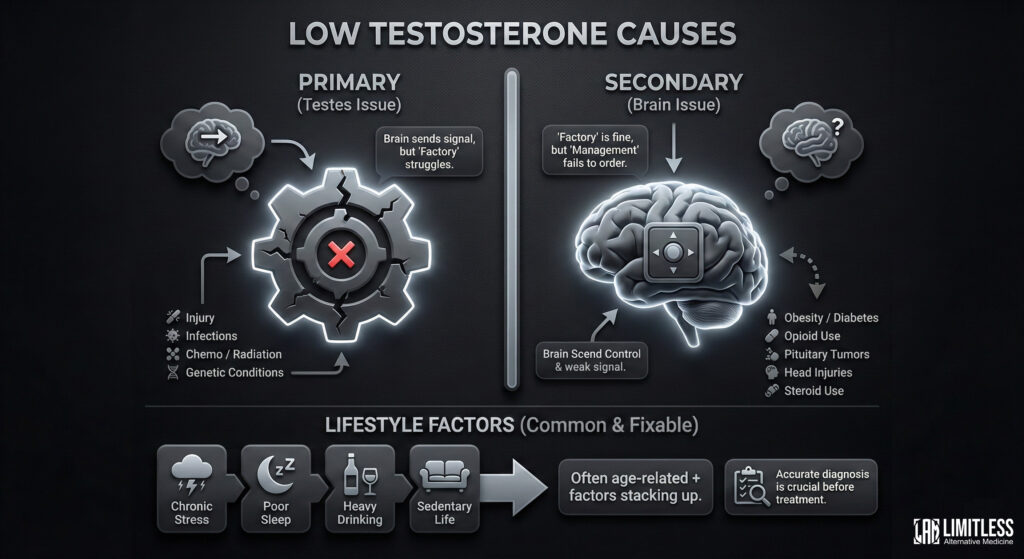
What Causes Low Testosterone?
The causes break into two camps, and the distinction matters because it changes how your doctor approaches treatment.
Primary hypogonadism
This means the problem is in the testes themselves. The brain is sending the signal, “Hey, make testosterone”, but the factory is struggling. Causes include testicular injury, infections like mumps orchitis, chemotherapy, radiation, or genetic conditions like Klinefelter syndrome.
Secondary hypogonadism
Here the factory is fine, but the management office (the hypothalamus and pituitary gland in the brain) isn’t sending the right orders. This can result from obesity, type 2 diabetes, chronic opioid use, pituitary tumors, head injuries, or—and this is a common one—prolonged use of anabolic steroids, which essentially teaches your brain to stop asking for natural production.
And then there are the lifestyle factors, which are both the most common and the most fixable: chronic stress, poor sleep, heavy drinking, and sitting around all day. In a lot of cases, low T is some combination of natural age-related decline plus these contributing factors stacking up over time. Which is why a good diagnostic workup is essential before anyone hands you a prescription.
For a deeper dive, See: Signs of Low Testosterone
How to Get Tested and Diagnosed
This is the part where you actually do something instead of just reading about it on your phone at 11 PM, so pay attention.
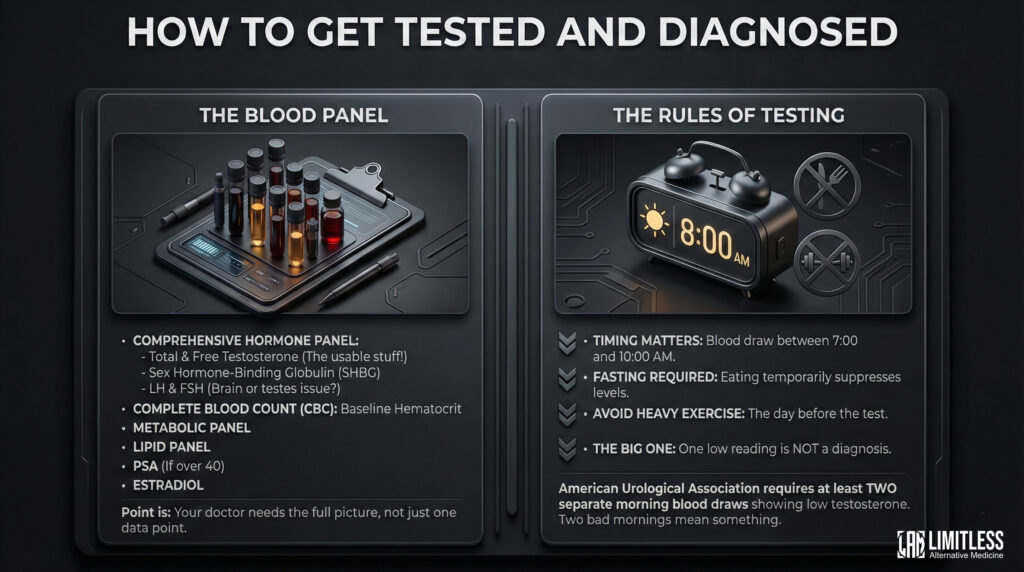
The Blood Panel
A responsible provider won’t just check your total testosterone and call it a day. You need a comprehensive hormone panel, which includes total testosterone, free testosterone (this is the stuff your body can actually use—total T includes testosterone that’s bound up and unavailable, like money in a retirement account you can’t touch), sex hormone-binding globulin (SHBG), LH and FSH (these tell your doctor whether the problem is in your brain or your testes), a complete blood count to establish your baseline hematocrit (this becomes important later), a metabolic panel, a lipid panel, PSA if you’re over 40, and estradiol.
That’s a lot of acronyms. The point is: your doctor needs the full picture, not just a single data point.
The Rules of Testing
Testosterone levels peak in the early morning and fluctuate throughout the day, which means timing matters. Blood should be drawn between 7:00 and 10:00 AM, fasting, because eating can temporarily suppress your levels. You should avoid heavy exercise the day before.
And here’s the big one: one low reading is not a diagnosis. The American Urological Association requires at least two separate morning blood draws showing low testosterone before confirming hypogonadism. One bad morning doesn’t mean you have a hormonal condition. Two bad mornings, on the other hand, starts to mean something.
How to Get a TRT Prescription
Alright, so your labs came back low. Twice. Your symptoms check out. Now what?
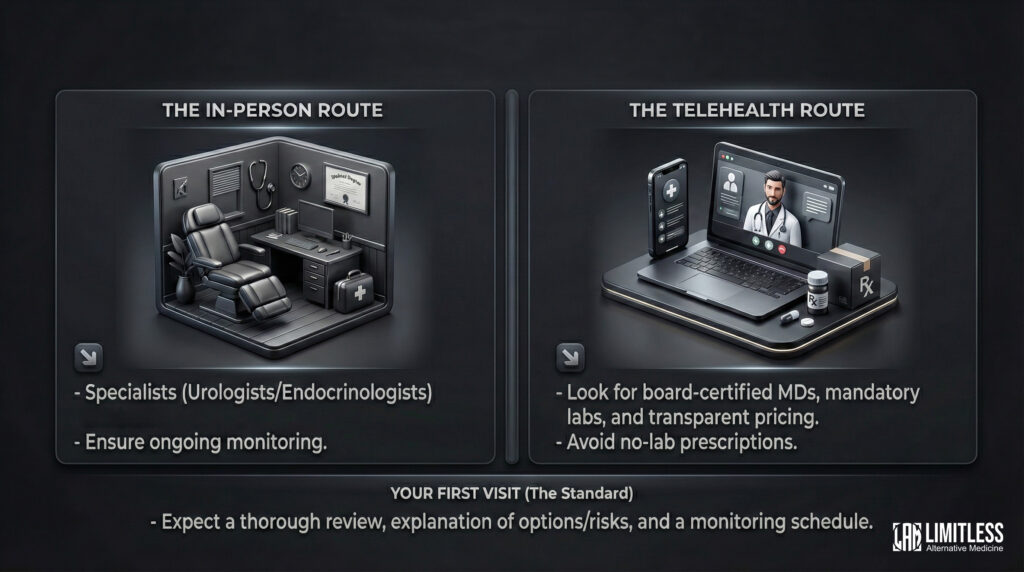
The In-Person Route
Urologists and endocrinologists are the specialists best equipped to manage TRT. Your primary care doctor can also prescribe it, though specialists tend to be more fluent in the nuances of dosing, monitoring, and the inevitable adjustments that come with dialing things in. The key thing to look for in any provider: do they monitor you after prescribing? A doctor who writes a script and sends you on your way is a doctor doing half the job.
The Telehealth Route
Online men’s health clinics have made TRT much more accessible, which is mostly good but also means you need to be discerning. The best ones handle lab orders, virtual consultations, prescriptions, and medication delivery in a streamlined package. The worst ones are basically prescription mills in a nice website’s clothing.
When evaluating a telehealth provider, here’s what to look for: board-certified physicians (not just nurse practitioners) making the prescribing decisions, mandatory lab work before they’ll prescribe anything, a commitment to follow-up blood work and ongoing monitoring, and transparent pricing. If a clinic is willing to prescribe testosterone to you without seeing lab results first, that is not a progressive clinic embracing modern medicine. That is a red flag.
Your First Visit
Whether you walk into an office or open a laptop, the first appointment should involve a thorough review of your symptoms, your medical history, your current medications, and your lab results. The provider should explain the different treatment options, walk through the risks and side effects without either minimizing or catastrophizing them, and set up a monitoring schedule. If any of that gets skipped, you’re at the wrong place.
See here for a detailed comparison of Telehealth Vs. In Person.
How TRT Works: Methods, Dosing, and What to Expect
Now we get into the practical stuff. There are several ways to get testosterone into your body, and the best method depends on your lifestyle, your tolerance for needles, and how your body responds.
Administration Methods
| Method | Frequency | Pros | Cons |
| Intramuscular Injections (Cypionate/Enanthate) | Every 1–2 weeks | Cheapest option, precise dosing, most clinical data | Self-injection, potential peaks and valleys |
| Subcutaneous Injections | 2–3x per week | Tiny needle, more stable levels | More frequent injections |
| Topical Gels/Creams | Daily | Steady levels, no needles | Transfer risk to others, pricier |
| Pellets (Testopel) | Every 3–6 months | Set it and forget it | Minor surgical insertion, hard to adjust |
| Patches | Daily | Consistent delivery | Skin irritation, can peel off |
Intramuscular injections of testosterone cypionate remain the most commonly prescribed method, mostly because they’re cheap, effective, and backed by decades of data. They’re the Toyota Camry of TRT delivery methods: not glamorous, totally reliable.
If you want a detailed comparison on administration methods: See here.
Typical Dosing
Most guys start on 100 to 200 mg of testosterone cypionate or enanthate per week, often split into two smaller injections (say, 80 mg Monday and 80 mg Thursday) rather than one big dose. Splitting the dose keeps your blood levels more stable, which means fewer side effects and less of that roller-coaster feeling where you feel great for three days and then like a wet blanket for four. Your provider will adjust based on follow-up labs, usually at the 6-week and 12-week marks.
When Will You Notice a Difference?
TRT is not a light switch. It’s more like a sunrise. Research published in the New England Journal of Medicine found: mood improvements tend to show up within 3 to 4 weeks—subtle at first, like you suddenly realize you didn’t need that third cup of coffee. Libido and sexual function typically improve within 3 to 6 weeks. Body composition changes—more muscle, less belly—take 3 to 6 months. Full bone density benefits take a year or two. The timeline depends on where you started, how consistent you are, and what else you’re doing (diet, exercise, sleep). TRT is not a substitute for those things. It’s the foundation that makes those things possible again.
Medical Oversight and Monitoring
This section is important and also, I’ll be honest, not the sexiest part of the guide. But it’s the part that separates responsible TRT from the kind of thing you look back on in five years and wince about.
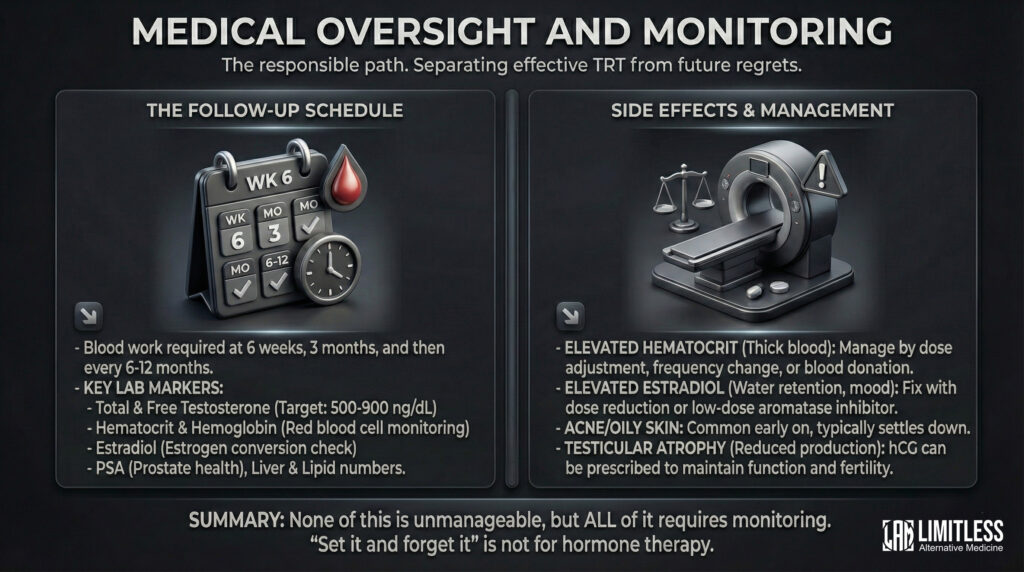
The Follow-Up Schedule
After starting TRT, you need blood work at 6 weeks (to check your initial response), at 3 months (for dose optimization), and then every 6 to 12 months for as long as you’re on therapy. According to The Endocrine Society’s clinical practice: total and free testosterone (aiming for 500 to 900 ng/dL, is the therapeutic sweet spot), hematocrit and hemoglobin (because testosterone stimulates red blood cell production, and too many red blood cells is a problem), estradiol (your body converts some testosterone to estrogen via a process called aromatization, and you need to keep that in check), PSA (prostate health), and your liver and lipid numbers.
Side Effects and What to Do About Them
Most TRT side effects are dose-dependent, which is a fancy way of saying they’re usually fixable by adjusting the dose. Elevated hematocrit is the most common issue—your blood gets too thick, essentially—and it’s managed by tweaking the dose, injecting more frequently in smaller amounts, or donating blood. Elevated estrogen can cause water retention, mood swings, or breast tissue tenderness; this usually resolves with a dose reduction or, in some cases, a low-dose aromatase inhibitor. Acne and oily skin are common early on and typically settle down. Testicular atrophy happens because when you supply testosterone externally, your body reduces its own production (the factory gets the memo that supply is covered and scales back). If fertility is a concern, your provider can prescribe hCG alongside TRT to keep things running.
The important point: none of this is unmanageable. But all of it requires monitoring. “Set it and forget it” works for rotisserie ovens. Not for hormone therapy.
What Does TRT Cost?
Let’s talk money, because this is always the question people are afraid to ask, so they just don’t, and then they’re surprised.
| Method | Estimated Monthly Cost (Without Insurance) |
| Testosterone Cypionate (generic) | $30–$80 |
| Topical Gel (AndroGel, Testim) | $200–$500 |
| Compounding Pharmacy Cream | $50–$120 |
| Pellets (Testopel) | $500–$1,000 per insertion (every 3–6 months) |
| Telehealth All-Inclusive | $150–$350 |
The most affordable route is generic testosterone cypionate picked up at your pharmacy with a GoodRx coupon. We’re talking under $30 for a vial that lasts two months. This is not an expensive medication. The expensive parts, if there are any, tend to be the telehealth subscriptions or the fancy delivery methods.
Insurance Coverage
Good news: many insurance plans cover TRT if you have a documented diagnosis of hypogonadism—meaning two blood tests confirming low testosterone plus clinical symptoms. That said, coverage varies wildly, so call your insurer and ask about formulary status for your specific medication, whether prior authorization is required, whether they cover monitoring labs, and whether they require step therapy (i.e., making you try the cheapest option before approving something else). Even with insurance, injectable testosterone is typically a low-cost generic, so your out-of-pocket is usually pretty modest.
Benefits, Risks, and the Bottom Line
What TRT Can Do For You
When administered properly and monitored responsibly, TRT has been shown to improve energy levels and reduce that soul-crushing fatigue, restore a healthy sex drive and erectile function, increase lean muscle mass while reducing body fat, sharpen mood, motivation, and cognitive clarity, support bone mineral density, and improve certain markers of cardiovascular health (though the long-term cardiovascular picture is still being studied).
That’s a meaningful list. For a lot of men, TRT is the difference between going through the motions and actually being present in their own lives.
Who Should Not Do This
TRT is not for everyone. You should avoid it if you have a history of prostate or breast cancer, untreated severe obstructive sleep apnea, uncontrolled heart failure, The Endocrine Society recommends monitoring hematocrit at baseline, 3 to 6 months, then annually, with dose adjustment if it exceeds 54%., or if you are actively trying to have a baby (exogenous testosterone suppresses sperm production, sometimes dramatically).
One piece of good news on the risk front: the TRAVERSE trial, published in the New England Journal of Medicine in 2023 and one of the largest randomized controlled studies on TRT, found that testosterone therapy did not increase the risk of major cardiovascular events in men with hypogonadism who had preexisting cardiovascular risk. This was a significant finding that has meaningfully reshaped the risk-benefit conversation around TRT.
The Takeaway
TRT is a legitimate, evidence-based medical treatment for men with clinically confirmed low testosterone. It’s not a miracle, and it’s not a shortcut. It’s a correction—a way of giving your body back what it’s no longer making enough of on its own.
Getting properly diagnosed requires fasting morning blood work, done twice. Multiple delivery methods exist, with injectable testosterone cypionate being the most cost-effective and well-studied. Ongoing monitoring is essential. Costs are manageable. Both telehealth and in-person providers can prescribe TRT, but the quality of care varies enormously, so choose someone who treats follow-up labs as non-negotiable, not optional.
If any of this resonated—if you’ve been feeling off and you can’t quite put your finger on why—the first step is simple and costs you nothing but an early morning and a blood draw. Get your levels tested. Have the conversation. You’ve been running on whatever version of yourself this is for long enough. It’s worth finding out whether there’s a better one available.
References
1. Mulhall JP, Trost LW, Brannigan RE, et al. Evaluation and Management of Testosterone Deficiency: AUA Guideline. American Urological Association. 2018.
2. Bhasin S, Brito JP, Cunningham GR, et al. Testosterone Therapy in Men With Hypogonadism: An Endocrine Society Clinical Practice Guideline. J Clin Endocrinol Metab. 2018;103(5):1715–1744.
3. Lincoff AM, Bhasin S, Flevaris P, et al. Cardiovascular Safety of Testosterone-Replacement Therapy (TRAVERSE). N Engl J Med. 2023;389(2):107–117.
4. Snyder PJ, Bhasin S, Cunningham GR, et al. Effects of Testosterone Treatment in Older Men. N Engl J Med. 2016;374(7):611–624.
5. Corona G, Giagulli VA, Maseroli E, et al. Testosterone Supplementation and Health: A Systematic Review and Meta-Analysis. Lancet Diabetes Endocrinol. 2017.
6. Cleveland Clinic. Testosterone Replacement Therapy (TRT). Cleveland Clinic Health Library. 2024.
7. Mayo Clinic. Testosterone Therapy: Potential Benefits and Risks as You Age. Mayo Foundation for Medical Education and Research. 2024.