

Why TRT Blood Test Requirements Matter for Safe Treatment
TRT blood test requirements exist because low testosterone shares symptoms with about two dozen other conditions. Depression. Thyroid dysfunction. Sleep apnea. Diabetes. They all do a very convincing impression of low T. Without proper bloodwork, your provider would essentially be guessing.
Learn more about the common symptoms of low testosterone and how they overlap with other conditions
There’s also a safety component that doesn’t get talked about enough. Reputable clinics won’t touch you without baseline labs because they need to know where you started. If six months down the road your red blood cell count spikes or your liver enzymes go haywire, they need that original data to compare against. It protects you. It protects them. It’s the boring, responsible thing that makes all the exciting stuff possible later.
The Endocrine Society’s Clinical Practice Guideline on Testosterone Therapy (the closest thing this field has to a bible) specifically recommends that hypogonadism should only be diagnosed in men who have both symptoms consistent with testosterone deficiency and consistently low serum testosterone confirmed on at least two separate morning draws. Two. Not one. Because even your hormones have bad days.
Complete TRT Blood Test Panel: Every Lab You Need
Here’s a quick-reference summary of every test in a full TRT blood test panel, followed by a detailed breakdown of what each one tells your doctor.
TRT Blood Test Requirements: Summary Table
| Test | What It Measures | Why It Matters for TRT |
|---|---|---|
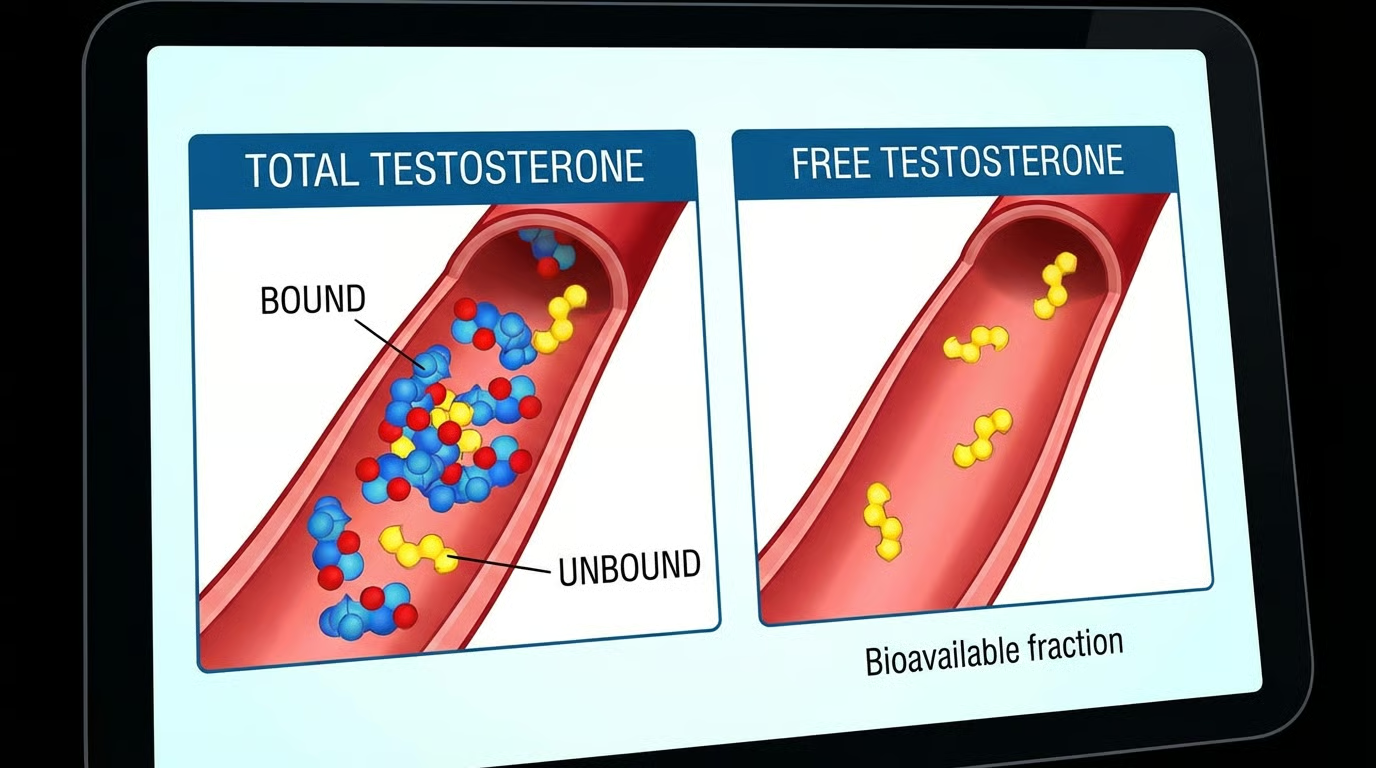
| Total Testosterone | All testosterone (bound + free) | Determines if levels are clinically low |
| Free Testosterone | Unbound, usable testosterone | Often low even when total T is “normal” |
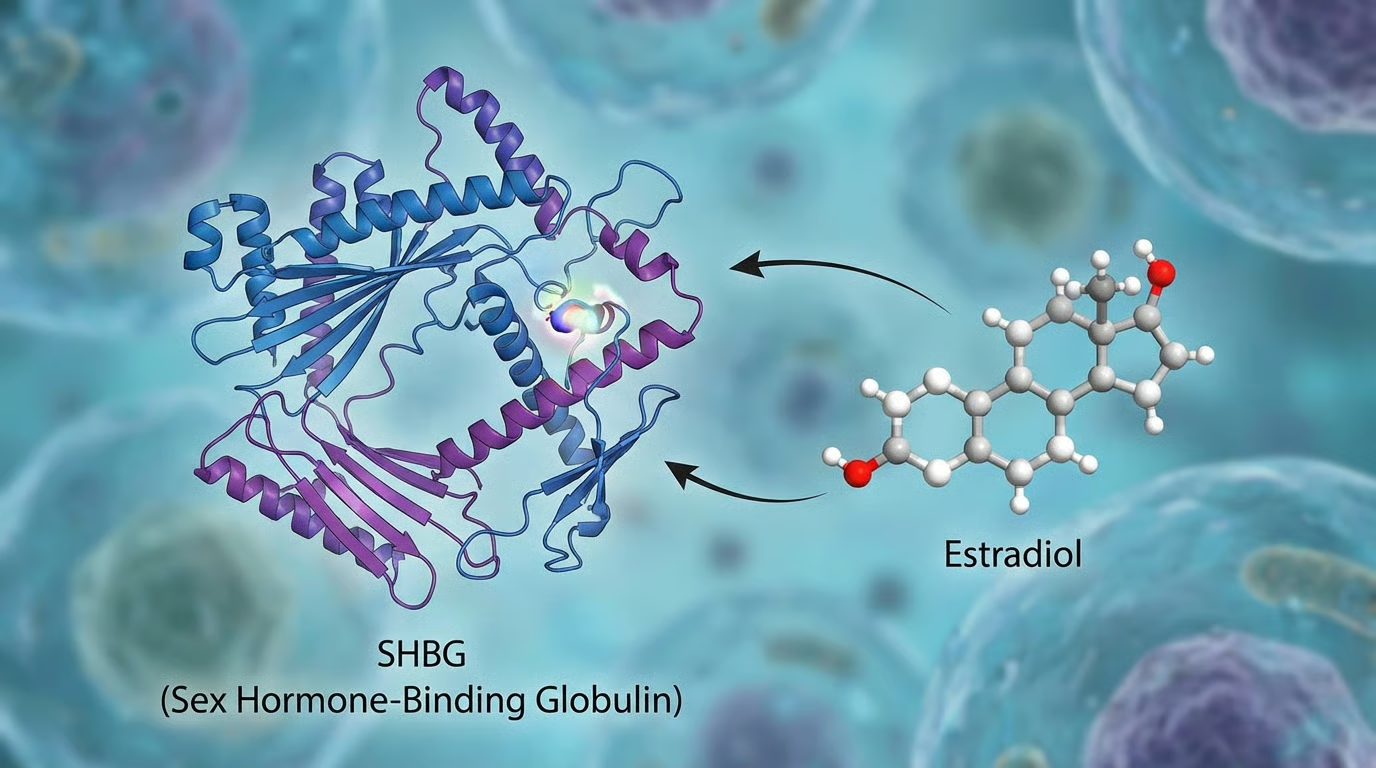
| SHBG | Protein that binds testosterone | Explains the gap between total and free T |
| Estradiol (E2) | Primary male estrogen | Baseline needed to manage aromatization on TRT |
| CBC (Complete Blood Count) | Red/white blood cells, hematocrit | TRT raises hematocrit — must monitor for clot risk |
| CMP (Comprehensive Metabolic Panel) | Liver, kidney, blood sugar, electrolytes | Confirms organs can safely process exogenous testosterone |
| Lipid Panel | Cholesterol and triglycerides | TRT can shift lipid profiles in either direction |
| PSA (Prostate-Specific Antigen) | Prostate health marker | Baseline needed to monitor prostate during treatment |
| LH & FSH | Pituitary signaling hormones | Distinguishes primary from secondary hypogonadism |
| Thyroid Panel (TSH, Free T3, Free T4) | Thyroid function | Rules out thyroid dysfunction mimicking low T |
| Prolactin | Pituitary hormone | Elevated levels suppress testosterone; may indicate adenoma |
| Vitamin D | Vitamin D status | Deficiency linked to lower testosterone production |
| Ferritin | Iron storage | Low iron causes fatigue often mistaken for low T |
Total Testosterone and Free Testosterone: The Core TRT Blood Tests
Total Testosterone is the headliner. This measures all the testosterone in your bloodstream, both the stuff bound to proteins and the stuff floating free. Most labs call anything between 300–1,000 ng/dL “normal,” but there’s an enormous, contentious, surprisingly emotional debate about what “normal” even means. A 35-year-old sitting at 310 ng/dL is technically in range. He’s also probably feeling like a phone at 4% battery. Context matters. A good provider looks at your number in relation to your age, your symptoms, your life. Not just whether it clears some arbitrary threshold.
Free Testosterone is, arguably, the more important number, and it’s the one a lot of providers forget. Only about 2–3% of your testosterone is actually “free,” meaning available for your body to use. The rest is bound to proteins like SHBG and albumin, just riding around doing nothing, like a guy on a bus who missed his stop and is too polite to say anything. You could have decent total testosterone and rock-bottom free T, and you’d still feel terrible. Make sure this is on your panel.
SHBG and Estradiol: The Hormones That Shape Your TRT Protocol
Sex Hormone-Binding Globulin (SHBG) is the protein that determines how much of your testosterone is free versus bound. High SHBG grabs your available testosterone and holds it hostage. Low SHBG can signal other metabolic issues. Either way, this number helps your doctor understand the full equation, not just the headline.
Estradiol (E2) is a form of estrogen, and yes, men produce it. When you start TRT, your body converts some testosterone into estradiol through a process called aromatization, which is a lovely word for something that can become not-lovely fast. Too much estradiol: water retention, mood swings, breast tissue growth. Too little: joint pain, brain fog, a general feeling of wrongness. Baseline levels help your provider calibrate treatment and decide whether you’ll need an aromatase inhibitor down the road.
Blood Health and Safety Markers Required Before Starting TRT
Here’s where we shift from “what’s your testosterone doing” to “can your body actually handle this.” These are the tests that keep you safe. They’re not glamorous. They will never be the subject of a podcast. They matter enormously.
CBC: The TRT Blood Test That Monitors Clot Risk
Complete Blood Count (CBC) matters, and here’s why: TRT stimulates red blood cell production. That’s a well-documented effect. Sounds fine, right? More red blood cells, more oxygen delivery, more vitality? Sure, up to a point. Past that point, your blood gets thicker. And thicker blood is not the win it sounds like. Thicker blood means higher risk of clots, stroke, cardiovascular events. The kind of things that make you wish you’d been more careful.
A 2022 study published in The Journal of Urology looked at data from over 74 million patients and found that men who developed secondary polycythemia (hematocrit at or above 52%) while on testosterone therapy had a 35% increased risk of major adverse cardiovascular events and venous thromboembolism in the first year of treatment. Thirty-five percent. That’s not a rounding error. That’s why your doctor needs a baseline CBC and why they’ll keep checking it.
Metabolic Panel, Lipids, and PSA: Organ Function Before TRT
Comprehensive Metabolic Panel (CMP) covers liver function, kidney function, blood sugar, and electrolytes. Your liver processes testosterone. If your liver enzymes are already elevated, if your liver is already, metaphorically, working a double shift, piling TRT on top would be reckless. Same for kidneys. These organs are doing hard, unglamorous, essential work. Your provider needs to know they’re up to the task before adding to their workload.
Lipid Panel checks cholesterol and triglycerides. Testosterone can shift your lipid profile, sometimes for the better, sometimes not. If you’ve already got borderline cholesterol, your doctor might want to address that before or alongside starting therapy. This isn’t gatekeeping. This is making sure you don’t solve one problem by creating another.
Prostate-Specific Antigen (PSA) is required for men over 40, and frankly it’s smart for anyone starting TRT. Testosterone does not cause prostate cancer. That old myth has been largely put to rest. But testosterone can accelerate existing prostate conditions, which is a meaningful distinction. A baseline PSA gives your provider a reference point for all future monitoring.
Additional TRT Blood Tests Most Clinics Skip
Here’s where you find out how good your clinic actually is. The budget operations check your total T, maybe your CBC, and call it a day. A thorough provider goes further. And you should insist on it, even if it means being the slightly annoying patient. Be the slightly annoying patient. Your health is worth a little social discomfort.
LH and FSH: Diagnosing the Cause of Low Testosterone
Luteinizing Hormone (LH) and Follicle-Stimulating Hormone (FSH) tell your doctor why your testosterone is low, which turns out to be a fairly important question. Is the problem in your testes (primary hypogonadism) or in your brain’s signaling system (secondary hypogonadism)? This distinction changes everything. Secondary hypogonadism might respond to clomiphene or hCG, potentially making TRT unnecessary altogether. Without LH and FSH testing, you’re skipping a diagnostic step that could save you years of injections.
Thyroid Panel: Ruling Out the Most Common TRT Misdiagnosis
Thyroid Panel (TSH, Free T3, Free T4) is one I feel strongly about. Thyroid dysfunction mimics low testosterone almost perfectly. Fatigue. Weight gain. Brain fog. Low libido. The overlap is uncanny. I’ve seen forum after forum full of guys who jumped on TRT when their real issue was hypothyroidism. A simple, inexpensive thyroid panel could’ve saved them months of unnecessary medication and the particular frustration of treating the wrong thing.
Prolactin: The Overlooked TRT Blood Test That Can Save Your Health
Prolactin gets overlooked with startling frequency. Elevated prolactin suppresses testosterone production and causes symptoms like low sex drive and, in some cases, breast tissue growth. Here’s the thing that makes this one urgent: high prolactin sometimes indicates a pituitary adenoma. That’s a benign brain tumor. It sounds terrifying, but it’s actually very treatable if you catch it. The Pituitary Society’s international consensus statement, published in Nature Reviews Endocrinology, notes that prolactinomas account for roughly half of all pituitary adenomas and respond remarkably well to dopamine agonist medications like cabergoline. But you have to know it’s there first. Don’t skip this test.
Vitamin D and Ferritin: Deficiencies That Mimic Low Testosterone
Vitamin D and Ferritin might seem like they wandered in from a different appointment, but they’re connected to testosterone production in ways that matter. Vitamin D deficiency is linked to lower testosterone levels. Low ferritin (your iron storage marker) causes fatigue that looks identical to low T fatigue. Sometimes correcting these deficiencies improves testosterone on its own. No injections. No protocol. Just your body working the way it wants to when you give it what it needs.
How to Prepare for Your TRT Blood Tests
You can’t roll out of bed at 3 PM, grab a large coffee, and expect your bloodwork to mean anything. How and when you get your blood drawn matters. A lot. Testosterone fluctuates throughout the day, and certain behaviors can tilt your results in directions that don’t represent reality.
Get your blood drawn in the morning. Ideally between 7 AM and 10 AM. Testosterone peaks in the early morning hours and can drop 30–40% by afternoon. Test in the evening and you might look hypogonadal on paper when you’re actually fine.
Fast for 8–12 hours beforehand. This isn’t just for the lipid panel. Eating can temporarily affect hormone levels too. Water is fine, and actually helpful (hydrated veins are cooperative veins). But skip the food, the sugary drinks, and definitely the alcohol the night before.
Sleep well the night before. This sounds like your mother talking, but she’s right. Poor sleep tanks testosterone levels temporarily. One bad night can drop your T by 10–15%. If you pulled an all-nighter or got four hours because anxiety about the appointment kept you staring at the ceiling, your results won’t reflect your real baseline.
Skip intense exercise for 24–48 hours before your test. Heavy lifting spikes testosterone temporarily, which sounds great until you realize it gives your doctor a falsely elevated reading. You want your resting baseline, the real number, not your post-deadlift peak.
Tell your doctor about everything you’re taking. Medications, supplements, all of it. Opioids and corticosteroids affect hormone levels. Biotin (which hides in a surprising number of men’s multivitamins) can actually interfere with lab assays and produce false readings. Full disclosure upfront saves everyone headaches later.
What Happens After Your TRT Blood Test Results Come Back
So you’ve done the bloodwork. You’ve waited the agonizing 3–7 days, which is enough time to convince yourself of approximately forty different diagnoses. Now you’re staring at numbers that may or may not make sense.
Your provider reviews the full panel, not just your testosterone number in isolation. They’re looking for patterns. Relationships. Stories the numbers tell when you read them together. Low total T plus low LH might point to a pituitary issue. Low free T with high SHBG tells a different story than low free T with normal SHBG. Elevated liver enzymes might mean you need additional workup before anyone talks about treatment. It’s all connected, and a good doctor treats it that way. For a deeper look at how these markers interact and why interpretation is more nuanced than simple reference ranges, the PMC review on challenges in testosterone measurement and data interpretation is an excellent resource.
Most providers will want two separate low testosterone readings before diagnosing hypogonadism. That’s not them being difficult. It’s standard medical practice. Testosterone fluctuates day to day based on stress, sleep, illness, whether you had a fight with your brother, whether the dog kept you up. A single low reading could be a fluke. Two confirms a pattern.
If your results confirm low testosterone, your provider will discuss treatment options based on your specific situation. TRT is not one-size-fits-all. Your age, fertility goals, other health conditions, and the type of hypogonadism you have all factor into the protocol they recommend. Some guys thrive on injections. Others prefer topical gels or pellets. The initial bloodwork guides that decision.
Once you start treatment, expect more bloodwork. Typically at the 6-week mark, then at 3 months, 6 months, and annually after that. Your doctor will track testosterone levels, hematocrit, PSA, liver function, and estradiol to make sure everything stays in a safe range. Ongoing monitoring is just as important as the initial TRT blood test requirements. Maybe more so.
TRT Blood Test Requirements: FAQ
What blood tests are required before starting TRT? A full TRT blood test panel includes total testosterone, free testosterone, SHBG, estradiol, CBC, comprehensive metabolic panel, lipid panel, PSA, LH, FSH, thyroid panel (TSH, Free T3, Free T4), prolactin, vitamin D, and ferritin. Some clinics only test total testosterone and CBC. That’s not thorough enough for safe treatment.
Why do I need two testosterone tests before starting TRT? Testosterone levels fluctuate from day to day based on sleep, stress, illness, and other factors. A single low reading could be an anomaly. The Endocrine Society recommends two separate morning blood draws with consistently low results before diagnosing hypogonadism and prescribing treatment.
What time of day should I get my TRT blood test? Between 7 AM and 10 AM, fasting. Testosterone peaks in the early morning and can drop 30–40% by afternoon. An evening test could show falsely low levels that don’t represent your actual baseline.
Do I need to fast before TRT blood work? Yes. Fast for 8–12 hours before your draw. This ensures accurate lipid panel and metabolic marker readings, and prevents food intake from temporarily affecting hormone levels. Water is fine and encouraged.
What testosterone level qualifies for TRT? Most guidelines use a total testosterone below 300 ng/dL as the threshold for diagnosing low testosterone, though the Endocrine Society and other organizations acknowledge that symptoms should be present alongside low lab values. A man at 310 ng/dL with real symptoms may still be a candidate depending on his free testosterone, SHBG, and overall clinical picture.
How often do I need blood tests after starting TRT? Typically at 6 weeks after starting, then at 3 months, 6 months, and annually thereafter. Your doctor will monitor testosterone levels, hematocrit, PSA, liver function, and estradiol to ensure treatment stays safe and effective.
Can TRT cause high red blood cell count? Yes. TRT stimulates red blood cell production, which can raise hematocrit levels. If hematocrit climbs above 52–54%, blood becomes thicker and the risk of blood clots, stroke, and cardiovascular events increases. This is why CBC monitoring throughout treatment is essential.
What if my testosterone is low but my doctor only checked total T? Ask for a full panel. Total testosterone alone doesn’t tell the full story. Free testosterone, SHBG, LH, FSH, and thyroid markers are all necessary to determine whether you truly have hypogonadism, what’s causing it, and what the right treatment approach is.
Final Thoughts on Meeting Your TRT Blood Test Requirements
I understand the impulse to skip ahead. When you feel lousy (truly, deeply lousy in that way where your own life starts to feel like something happening to someone else) the last thing you want is another obstacle between you and feeling better. Another appointment, another copay, another week of waiting.
But meeting your TRT blood test requirements isn’t an obstacle. It’s the opposite. It’s the thing that makes everything that comes after work. These labs confirm you actually need therapy, that your body can handle it safely, and that your provider has the data to get your protocol right. Not approximately right, but right for you, specifically, in your particular body with its particular history.
Don’t cut corners on this. Find a provider who runs full panels, not just a total testosterone check. Ask questions about every test they order. Ask questions about every result they explain. You are, after all, putting a powerful hormone into your body, into the only body you will ever have, and you deserve to go in understanding exactly where things stand.
Your TRT blood test requirements are your roadmap. They tell you where you’re starting. They help your doctor chart the course. They give you benchmarks to measure whether this whole thing is actually working. Treat them as the foundation they are, and you’ll be set up for the best possible version of what comes next.
Which, if you’re lucky and careful and willing to do the boring parts, might just be pretty good.